The ANZMES AGM was held at 1pm on the 18th November 2023 via ZOOM online meeting.
This was ANZMES 43rdAGM of caring and supporting people with ME/CFS and their whanau and carers, as well as disseminating information, resources, and education to them, the general public, and medical professionals. ANZMES is looking at new initiatives as part of our strategic planning for the next year, and will continue to fund vital research that benefits the ME/CFS community as more physiological evidence is discovered and more understanding of the condition is brought to the fore.
Fiona Charlton (President) opened the AGM Meeting and the President’s report outlined some of ANZMES activities throughout the year.
Highlights included;
This year we are proud to have launched a Grant and Scholarship Programme for postgraduate students and academic researchers. This will be an annual fund for ME/CFS and long COVID study. Two exciting projects are proceeding thanks to the ANZMES Grants of $25,000 each
ANZMES launched Know M.E. Series for health professionals providing a monthly newsletter packed full of evidence-based information and research. The associated video podcasts are publicly available. This series is CME accredited by the Royal NZ College of GP’s, and ANZMES is a Registered Provider for continuing medical education. This series features a newsletter covering a different topic each month. Know M.E. also includes a podcast which is publicly available on Spotify, iHeart Radio, Google Podcasts, and iTunes/Apple. The video version is publicly available on YouTube. Each month features special guest interviews speaking about M.E. topics.
In May 2023 ANZMES launched two one-page resources for the diagnosis and management of ME/CFS and long COVID in primary care.
In early November 2022 we held a long COVID educational event for health professionals. We had over 150 registrants, including GPs, nurses, nurse practitioners, clinic managers, med students, physiotherapists, OTs, and more. Our speakers talked about post exertional malaise and how to avoid it, described the similarities and differences between Long COVID and ME/CFS, how to diagnose both conditions, how to treat through allied health, and the effects of COVID and Long COVID in Māori and Pasifika communities.
Dr Sarah Dalziel attending the the 3rd ME/CFS International Conference 2023: RID – Research Innovation and Discovery and provided a summary of the conference.
All present committee member’s have continued their term and were voted on for the upcoming year. The appointments are as follows:
President – Fiona Charlton
Vice President – Ange Robinson
Treasurer – Amy Ma
Reviewer – Alan Shanks
Executive committee – Anna Brooks, Suzanne Duffy, Wendy Matthews, Steve Murray, Gabby Shortt and Ros Vallings.
Heather Wilson who has been on the ANZMES committee for well over 20 years has now stepped down. A very, very special thanks go to Heather for her hard work and time spent on the committee and time spent helping people and their whanau, it is much appreciated. After the AGM was announced closed a presentation was played of Heather’s farewell which was held online and in person in Dunedin on Friday 3rd November 2023.
Dr Sarah Dalziel and Ken Jolly both continue as ex officio Medical Advisor’s to ANZMES. We would like to sincerely thank Sarah and Ken for their time and effort to help answer any queries we may have in the medical field.
Membership Fees for 2024 have remained unchanged, they are set at:
$10.00 for Full membership
$5.00 for Concessionary membership
$5.00 for Family members
A free Helping Hand option will be available for people who suffer severe financial hardship.
After the AGM had finished, Dr Sarah Dalziel gave a presentation on her attendance at the 3rd ME/CFS International Conference 2023: RID – Research Innovation and Discovery.
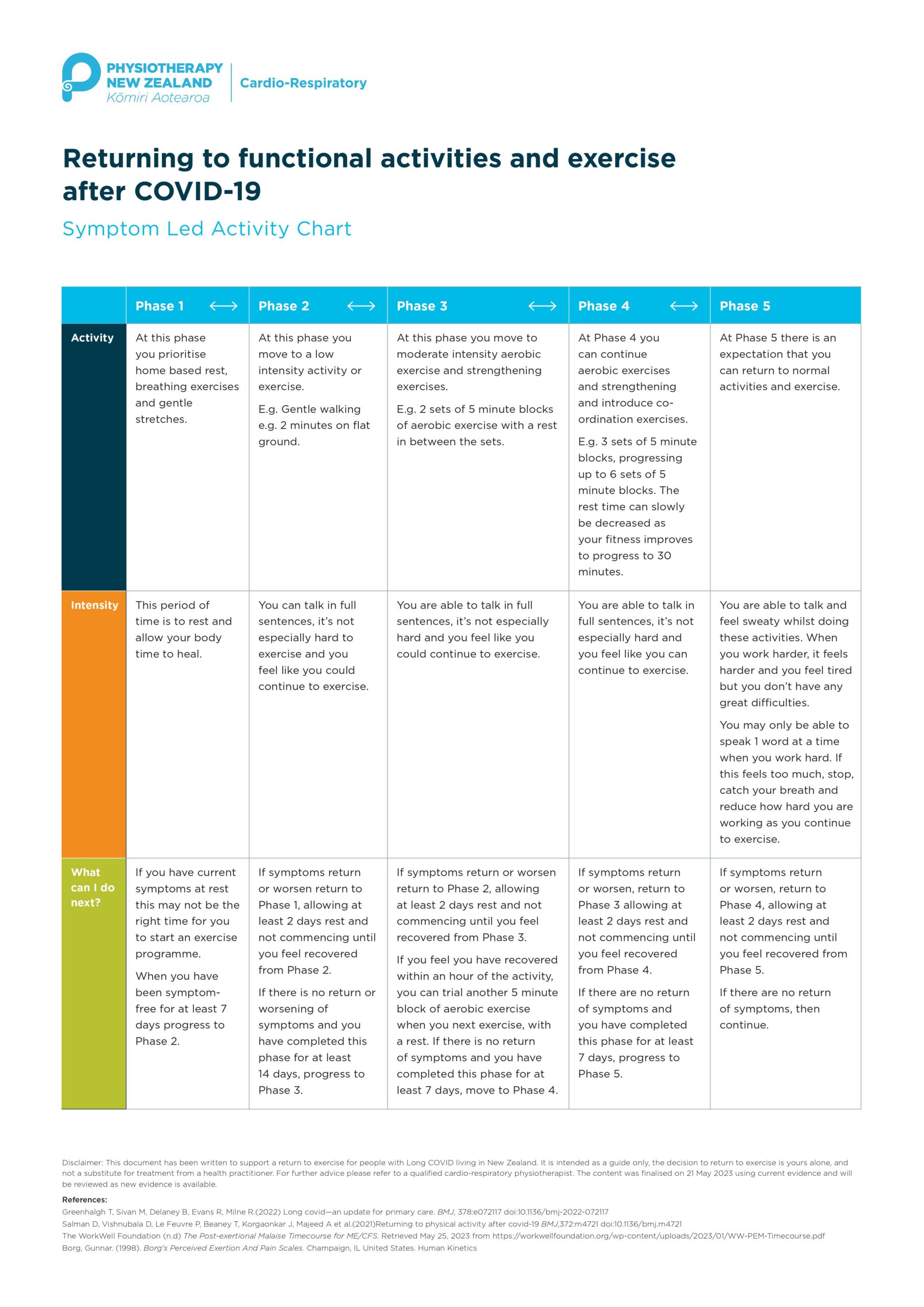
Physiotherapy New Zealand has provided ANZMES with a flow chart for the return to exercise advice in the Long COVID space. Please find attached the flow chart designed for health care professionals to be supported in giving safe exercise advice.
Two New Zealand researchers have been chosen to receive the Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) annual grant of $25,000 to undertake vital research into increasing understanding of Myalgic Encephalomyelitis (ME, also known as Chronic Fatigue Syndrome), in Aotearoa.
ANZMES, the National Advisory on ME, launched the new grant and scholarship programme for postgraduate students and academic researchers this year – aimed at supporting those interested in researching ME and long COVID. With six funding opportunities available, ANZMES encouraged applications from those seeking to undertake research that furthers understanding, treatment, or prevention of ME and long COVID, including two $25,000 grants and four $5,000 scholarships to support research and study costs.
The 2023 Grant recipients are: ● Principal investigator: Dr. Nicholas Bowden, Research Fellow, Department of Women’s and Children’s Health, University of Otago (pictured below. Photo credit: University of Otago).
Co investigators: Keith McLeod, Associate Principal, Kōtātā Insight. Dr. Rosamund Vallings, retired GP, Howick Health and Medical Centre. Emeritus Professor Warren Tate, Department of Biochemistry, University of Otago. Professor Barry Taylor, Department of Women’s and Children’s Health, University of Otago. Francisca Anns, PhD Candidate, COMPASS Research Centre, University of Auckland.
The study will investigate the health, labour market, and social service use of people with ME, in NZ, through a population study. Dr. Bowden says, “we are excited and grateful to receive this grant to undertake what we believe is an important piece of research, providing foundational population-level evidence on health, labour market, and social service outcomes for those with ME/CFS in Aotearoa/New Zealand for the first time.”
● Principal investigator: Dr. Lynette Hodges, Senior Lecturer School of Sport, Exercise and Nutrition, Massey University, Registered Clinical Exercise Physiologist (pictured below. Photo credit: Massey University).
The study will investigate activity and energy management and the hallmark symptom post-exertional malaise (PEM), in people with ME through an observational study that assesses exertion during normal daily activities of living, such as doing dishes or laundry.
Dr. Hodges says, “I am so thrilled to learn that my research application was chosen. I hope that this research will be able to be of benefit to those with ME/CFS. As a Clinical Exercise Physiologist, I am keen to help people live their best lives and hope that this study will develop a better understanding of how activities of daily living affect the physiology of those living with ME/CFS.”
Dr. Bowden and Dr. Hodges will both receive the $25,000 Grants through their respective universities, to carry out their research projects.
ANZMES President, Fiona Charlton, says, these investments will help facilitate a crucial source of New Zealand based research, furthering our understanding of the disabling condition.
“We are really pleased by the calibre of the work proposed by both recipients. “With Dr. Bowden’s work, for the first time we will have a foundational study that offers insight into the lives and experiences of people with ME in Aotearoa.
“We understand the burden of disease from an international research perspective but New Zealand based studies are lacking.
“Research into PEM and activity management will also be invaluable for both patients and health professionals and will have implications for long COVID management and recovery.
“While we did not receive any scholarship applications, we encourage postgraduate students to consider their Masters/PhD topics now, for next year’s funding round. In programs with relatively low costs, scholarships can be used to help pay fees or study and living expenses,” says Charlton.
ME is a complex, debilitating and often misunderstood medical condition and although millions of people suffer with the illness worldwide, including a significant population in New Zealand, there is remarkably little research or funding available.
This ANZMES funding programme was made possible by the generous support of members.
The Grant was awarded by ANZMES on the recommendation of their Grants and Scholarships Subcommittee.
Next year’s funding applications open May 31st. Visit anzmes.org.nz for more information, grant regulations, and application forms.
What is ME/CFS? Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is often triggered by a viral illness and involves overwhelming fatigue and other symptoms that range in severity as it affects many body systems, such as the immune, neuroendocrine and autonomic nervous system. The key characteristic of ME/CFS is post exertional malaise (PEM) which presents 12-48 hours after exertion, and can result in days to weeks of exacerbated symptoms. For the very severe, this exertion can be simply trying to speak, or eat.
Who are we? We are the National Advisory on ME in Aotearoa/New Zealand. With four decades of knowledge and experience, we are the trusted leaders in ME education, representation, and research. Our expertise comes from a reputable medical team of advisors, including a world renowned expert and MNZM recipient, a fellow of the Royal NZ College of General Practitioners (RNZCGP) and a network of academic researchers, clinicians, and representatives from the ME community. The executive committee comprises experts in their respective fields for governance, policy, leadership, representation, and education.
Always a trail-blazer, it was the first ME charity of its kind in the world, established in 1980, as ANZMES, to provide support, information dissemination, and representation, achieving past outcomes through dedication, passion, time, and knowledge of lived experience. Today, the organisation leads as a Royal New Zealand College of General Practitioners (RNZCGP) Continuing Medical Education (CME) Registered Provider, proud funder of vital research, and steward of the community voice. We continue to disseminate evidence-based information nationally, and represent the ME voice globally as a founding member of the World ME Alliance through advocacy and leadership. ANZMES latest education programme for health professionals – Know M.E. – is a video podcast and news series featuring up-to-date, evidence based research and information on ME and Post COVID Conditions.
ANZMES Launches New Grant and Scholarship Programme to Boost ME/CFS and long COVID Research
ANZMES, New Zealand’s national advisory for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), is pleased to announce the launch of a new grant and scholarship programme for postgraduate students and academic researchers. The programme is aimed at supporting those who are interested in researching ME/CFS and long COVID.
There will be six funding opportunities awarded each year to Postgraduates who undertake research that furthers understanding, treatment, or prevention of ME/CFS and long COVID, including two $25,000 grants to support laboratory research studies and four $5,000 scholarships to support students undertaking research projects. Academic researchers can also apply for the grants.
ME/CFS is a debilitating chronic condition involving overwhelming ongoing fatigue. Although millions of people suffer with the illness worldwide there is remarkably little research or funding available.
ANZMES President, Fiona Charlton, says “we are excited to launch this new programme, which aims to support the next generation of researchers and innovators to build a vital source of New Zealand based research, contributing to knowledge and scientific progress that will benefit the community.
“Promoting and investing in ME/CFS-focused research is a core objective of the organisation. Our funding programme is made possible by the support of our members.”
Two grants are being offered for postgraduate studies or academic research in either the Faculty of Science, Faculty of Medical and Health Sciences, Faculty of Public Health, or Faculty of Sport and Exercise Science to contribute towards the costs of laboratory analysis for a research project on ME/CFS or ME/CFS and long COVID.
Four scholarship awards will be offered each year to students to contribute towards the expenses of studying for a postgraduate degree in the Faculty of Health Sciences, Public Health or Humanities/Social Sciences for a student who can demonstrate financial project cost requirements or study expenses and who are conducting study/research on ME/CFS or ME/CFS and long COVID.
Applicants will be selected by ANZMES on the recommendation of their Scholarships Subcommittee.
The Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) supports the new position paper on the Lightning Process by the World ME Alliance and does not endorse the Lightning Process for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).
The Lightning Process is a programme loosely based on concepts of neuro linguistic programming (NLP) and cognitive behaviour therapy (CBT) that is set up commercially and currently marketed as a cure for ME/CFS. This claim is not backed by scientific evidence and ANZMES shares the view of the World ME Alliance that the promotion of this programme is likely to do harm.
The National Institute for Health and Care Excellence (NICE), in the UK, revised their guidelines for the diagnosis, treatment, and management of ME/CFS stating that the lightning process should not be used as a treatment and they no longer recommend CBT. These changes reflect a shift from an outdated perspective that ME/CFS was a psychological condition and follows evidence from over 200 studies showing poor efficacy for this treatment approach.
ANZMES President, Fiona Charlton says, “there is a growing body of evidence that shows that ME is driven by physiological changes not psychological ones and telling people that they can talk themselves out of this condition, within three days, could be very harmful.
“We know that if people with ME ignore their symptoms and push themselves this can make things worse, sometimes to the point of needing hospital care.”
ANZMES agrees with the World ME Alliance who highlight in their statement that people with ME/CFS are vulnerable to exploitation due to a lack of effective treatment where programmes like the Lightning Process are just filling this void.
People living with Long COVID are also being drawn into this treatment as this is now an extension of their claims to cure ME/CFS.
Other concerns with the Lightning Process include a bias in efficacy studies, including conflicts of interest, a reported secrecy where participants are told not to speak about the programme or their symptoms and a level of shame and guilt for those who do not recover within the three days of treatment.
Charlton says, “we want to ensure that if we are endorsing a treatment for ME that robust evidence supports efficacy and this is just not the case with LP.
“What we do know is that a treatment approach that is focussed around symptom management is shown to help with the relapsing nature of ME.”
ANZMES acknowledges that neurological symptoms, such as depression and anxiety can be a part of ME/CFS and may benefit from supportive therapies but people have the right to unbiased, impartial information when being offered these treatments.
***********************
The Lightning Process was developed and trademarked by British osteopath and hypnotherapist Phil Parker.
ANZMES has been providing information, building awareness, funding research, and advocating for people with ME/CFS for the past 42 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice, globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership.
At the request of the ME/CFS community, ANZMES has issued a survey relating to reactions experienced by the community to the COVID-19 Pfizer BioNTech vaccine. ANZMES also sought to ascertain prevalence of Long COVID and COVID-19 infection in the community. The opportunity was also utilised for respondents to express interest in participating in a potential fractionated dosing trial.
This report contains preliminary findings for responses received from 21st October 2021 to 10th November 2021. This survey is still open to capture experiences after these dates, as vaccination decisions are ongoing.
Please note that this survey is classed as a self-report questionnaire which seeks to ascertain the subjective experience of people with ME/CFS and co-morbid conditions. The information collected is therefore anecdotal data. No clinical research has been conducted.
Respondents
395 respondents identify with an ME/CFS diagnosis
144 with Fibromyalgia (some overlap with ME/CFS)
19 with COVID-19
5 diagnosed with, and 32 suspect, Long COVID
The majority of respondents have a clinical diagnosis of ME, with 25 self-diagnosed. Most are unsure as to which diagnostic criteria for ME was used.
Some questions have less respondents, therefore numbers are indicated in the relevant sections.
Functional capacity (pre-vaccination)
32.3% (144 individuals) are unable to work, confined to their home with a lot of rest required.
25.8% (115) are able to work part-time at home.
25.5* (115) are able to work part-time outside of the house.
9.9% (44) are able to work full-time with mild-moderate symptoms with activity. 1.1% (5) are able to work full-time without symptoms. * These respondents were mostly COVID-19 infection or Long COVID respondents without ME/CFS.
4.3% (19) are bedbound most of the time.
0.9% (4) are bedbound and unable to care for themselves.
Vaccination rates
The majority of respondents have had two doses of the Pfizer vaccination.
64.5% (296) two doses.
16.1& (74) single dose.
19.2% (88) have not been vaccinated.
Of the 296 with two doses, the duration between doses was 6 weeks or more for 166 individuals and 3 weeks for 130.
Pattern for capacity and reaction
These findings suggest that the more disabling the ME/CFS symptoms, the more prone to a relapse after vaccination but that relapse can occur at any functional capacity state for pwME. This was analysed when there were 241 responses.
Temporarily worsened
Improved
No change
Worsened into relapse
Worsened beyond illness
Not vaccinated
No answer
Part-time work home
22
8
7
9
1
14
2
Part-time outside house
22
3
17
14
0
12
2
Full-time work mild-mod with activity ME FM Long COVID/COVID
3 2 0
0 0 2
4 1 3
3 1 0
0 0 0
2 0 1
2 0 5
Unable to work, confined to house
23
6 3 temp
15
18
7
8
7
Bedbound mostly
2
0
0
3
0
1
1
Bedbound unable to care for self
0
0
0
1
0
1
1
Overall ME
72
20
43
48
8
30
20
First dose vaccination reaction and duration
There were 39 individuals who did not experience any symptoms. For those who did experience reactions to the first dose of the vaccine, these were consistent with the expected normal immune response, e.g.:
sore at injection site (300)
tired/fatigued (219)
Headache (142)
nausea/gastrointestinal issues (62)
fever/chills (56)
Swollen lymph nodes (46)
Sleep issues/insomnia (44)
5 people experienced heart palpitations and/or anxiety 3 people experienced skin sensitivity and/or allergy flares, with 2 people experiencing brain fog/cognitive issues.
For most people (130) these symptoms lasted 1-2 days.
For 93 individuals it lasted 3-6 days.
44 experienced symptoms for 7-14 days.
35 for over 2 weeks.
37 have not recovered.
Second dose reaction and duration
As has been reported by the general public, the findings from this survey suggest that pwME also experienced more adverse reactions to the second dose of the Pfizer vaccine. However there were 54 individuals who did not experience any symptoms.
For 97 individuals these symptoms lasted 1-2 days.
For 78 individuals it lasted 3-6 days.
26 experienced symptoms for 7-14 days.
20 for over 2 weeks.
44 have not recovered.
Vaccine effect on state of illness/wellness for 359 respondents
137 (38.1%) experienced no change/stay the same
118 (32.9%) temporarily worsened but have returned to baseline
71 (19.8%) worsened and not returned to baseline – relapsed
22 (6.1%) improved
11 (3.1%) worsened beyond anything experienced in illness to date – severe relapse
289 respondents did not have any new symptoms that they could attribute to the vaccine.
52 stated that they had new symptoms that they could attribute to the vaccine. These symptoms tended to be over-activation of the immune response, e.g. sore throat, swollen neck glands, allergy reactions. Of these 52 – 4 individuals have gastrointestinal issues, 2 experienced more fatigue whilst 1 indicated improved energy.
Clinical care
From 383 responses 314 (82%) were not offered clinical care during vaccination, 15 (3.9%) were offered clinical care, 19 (5%) were unsure. 25 people asked for specific clinical care during the vaccination process. Of those offered clinical care the options were 30 minute observation rather than the normal 15, separate areas with direct nurse observation. Others were advised by their GPs to rest and take antihistamines pre- and post-vaccination.
Caregiving requirements
From 353 respondents 50 require ongoing caregiving for their ME/CFS and/or FM and 70 required care after vaccination. 244 people do not require caregiving before and 230 after.
Fractionated dosing interest
If fractionated / lower dosing had been an option, of 115 responses 48 stated they would have considered it, 23 said they would not consider it and 44 were unsure.
Of 88 responses for those reluctant to have the vaccine, 57 would consider lower dosing options, 10 would not, and 21 were unsure.
Of 124 responses to indicate interest in participation in a potential trial into fractionated dosing, 61 responded that they are interested, 31 may be interested, and 32 are not.
Antihistamine usage
Of 115 responses 45 did not take any pre- or post-vaccination, 70 did.
Reasons for not being vaccinated
Of 1Anxiety/worry/fear about potential adverse reactions, previous adverse reactions to other vaccines, concern about the safety of the vaccine, high ME/CFS symptomatology, chemical sensitivities/MCS/MCAS, not currently well enough to risk adverse reactions.
COVID-19 / Long COVID
19 respondents have been diagnosed with SARS-CoV-2 (COVID-19) infection.
169 respondents have had COVID-19 tests.
5 people have been diagnosed by a medical professional with Long COVID.
32 people suspected they have Long COVID after a viral infection due to ongoing or lingering classic COVID-19 symptoms and having been connected to a location of interest, an overseas hot zone of infection, or have remained unwell after experiencing a viral infection that has not been confirmed as COVID but has the same symptoms.
One of the primary objectives of ANZMES (Associated New Zealand Myalgic Encephalomyelitis Society) is to further the cause of ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome) through the promotion and funding of research into the disease. The global COVID-19 (SARS-CoV-2) pandemic has changed the way the world operates, interacts, and deals with new viruses. Yet the notion of post-viral syndromes is nothing new. People with ME/CFS who remain in a ‘state of dis-ease’ after glandular fever (Epstein Barr/mononucleosis) will attest to this. Likewise, an estimated 30% of people who had COVID-19 infections have not returned to their pre-illness state of health. This rising problem recognised by health professionals worldwide was initially coined as Long-hauler then Long COVID. The World Health Organisation (WHO) recently released a Clinical Case Definition, further acknowledging the problem faced by millions globally. The current WHO case definition states that:
“Post COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include fatigue, shortness of breath, cognitive dysfunction but also others which generally have an impact on everyday functioning. Symptoms may be new onset, following initial recovery from an acute COVID-19 episode, or persist from the initial illness. Symptoms may also fluctuate or relapse over time. A separate definition may be applicable for children.”
As previously highlighted in the ANZMES May 2021 press release for ME Awareness Day, there are striking similarities between the symptoms experienced by people with Long COVID and the symptoms experienced by people with ME/CFS. Besides the three mentioned in the WHO definition above, there are also flu-like symptoms (fevers/chills, muscle/joint aches/pains, headache, swollen lymph nodes) and gastrointestinal issues. These symptoms seem common in people experiencing post-viral syndromes, and yet people with ME/CFS and Long COVID experience additional symptoms unique to their conditions. For example, many with ME/CFS also endure autonomic dysfunction (dysautonomia, orthostatic intolerance), neuroendocrine malfunctions (cold extremities, intolerance to extreme heat/cold), immune over-activation (sensory, chemical, and environmental sensitivities) and other symptoms related to neuroinflammation and metabolic dysfunction. Those with Long COVID can be prone to depression or anxiety as a direct result of being chronically ill and may also have organ damage caused by the SARS-CoV-2 virus. Science and medicine still have much to learn about both conditions. For instance, why do some people contract COVID-19 and recover within a few weeks whilst others develop a persisting post-viral condition? Many of those infected in the first wave of the pandemic remained unwell more than 19 months later. Is the virus still present and active in the body or has the immune system gone haywire – stuck in a loop of search and destroy? Why does the immune system malfunction? What clues can the molecular structure of people with ME/CFS provide that may answer these questions for those with Long COVID? How can understanding Long COVID help people with ME/CFS?
These questions and more are the focus of a new study currently underway in New Zealand by co-investigators Dr. Anna Brooks, Senior Lecturer (School of Biological Sciences, Faculty of Science, University of Auckland) and Emeritus Professor Warren Tate (Department of Biochemistry, University of Otago) with Dr. Rosamund Vallings from Howick Health & Medical Centre as the key clinical investigator. ANZMES is pleased to provide partial funding for this research. Seed funding has also been awarded by Dr. Brooks’ department, Faculty, and the Maurice Wilkins Centre, a Centre for Research Excellence. However, most of the funding has been obtained via crowdfunding hosted by the University of Auckland Foundation. This funding avenue is still open and accepting donations: http://bit.ly/3AuTiYN
Dr. Anna Brooks Photo credit: University of Auckland
Emeritus Professor Warren Tate Photo credit: University of Otago
Dr. Brooks states “There is an urgent need to improve our understanding of the underlying biomedical mechanisms and immune dysfunction associated with Long COVID and other post-viral diseases. Already research is beginning to reveal the similarities between certain lingering symptoms following COVID-19 illness and ME/CFS. Patient groups are now strongly advocating for biomedical research on Long COVID to be collaborative, multidisciplinary and importantly, draw on the experience of those who have been investigating biomedical causes and mechanisms of ME/CFS.”
The experience Dr. Brooks refers to is that of Prof. Tate, winner of the Rutherford medal in 2010, who has been investigating ME/CFS since 2012, and has identified molecular signatures of ME/CFS. As co-investigators for this new study, Dr. Brooks and her team are conducting immunological studies and Prof. Tate and his team are performing molecular studies of Long COVID and its relationship to ME/CFS. Prof. Tate aims to perform molecular analyses on a subgroup of this study in addition to providing samples from his ME/CFS patient group for analysis of immunological status before and after vaccination. In addition to being an experienced cellular immunologist, Dr. Brooks is also Director of Auckland Cytometry, the core facility which houses the leading-edge technologies necessary to perform these critical analyses.
How will this research benefit the ME/CFS community? Since a certain percentage of people with Long COVID symptoms also fit the diagnostic criteria for ME/CFS and many go on to receive this diagnosis as well, the samples analysed as part of this study will be beneficial in tracking early onset ME/CFS in comparison to Long COVID. It is hoped that the researchers will be able to identify key markers of immune dysfunction, especially as a percentage of samples will be obtained at very early stages of disease. This investigation into the unique immune signature of ME/CFS and Long COVID has the potential to unveil a biomarker specific to these conditions. As Dr. Brooks’ core expertise is with advanced flow cytometry, this research will screen for over 100 immune cell biomarkers which to date supersedes any previously screened for in ME/CFS research. “This will be a world first.” states Dr. Brooks.
ANZMES is proud to play a part in this exciting new research endeavour into ME/CFS and Long COVID and will continue to update the community with news as the study progresses. As always, ANZMES welcomes donations which enable continual contributions towards vital and potentially life-changing research: www.anzmes.org.nz.
We have received many queries from our membership about COVID-19 Pfizer vaccination effects for people with ME/CFS in New Zealand.
To answer these questions confidently and comprehensively we decided to create a self-report survey which asks you about your experience with the vaccine. Whether you’ve experienced mild, moderate, severe, or no effects, we would like to know. If you have chosen not to get the vaccination we would still like you to respond. If you are too unwell to fill out the survey yourself, you can ask someone else to fill it out on your behalf.
This survey also features questions regarding experiences and diagnoses of Long COVID as we seek to understand the prevalence and similarities to ME/CFS.
We hope many will participate in this vital research survey. If you require a survey sent by post, please let us know.
ANZMES asks experts for their recommendations on whether people with ME/CFS (pwME/CFS) should get the COVID-19 vaccine or not.
Dr. Ros Vallings, Howick Health & Medical Centre
COVID-19 can be a severe and debilitating disease which can lead to multi-organ damage and death in some people. If someone with ME/CFS catches COVID-19 it is likely to cause a significant exacerbation or relapse of their ME/CFS symptoms, as has been shown in the UK. Yet those experiencing a heightened immune system may be protected against catching viruses – although there is no guarantee. The Pfizer vaccine that is being administered in New Zealand is well studied and exceptionally safe and provides a high degree of protection. However, as with any vaccine some people with ME/CFS have an exacerbation of symptoms which overlap with the commonly reported side effects of the COVID-19 vaccines. A small percentage of people may have a more severe exacerbation of symptoms. I have many of my ME/CFS patients immunised now and not one has had a bad reaction to date. This may be because they used Dr. Nancy Klimas’ antihistamine suggestions which I recommend. I also provide a prescription for prednisone for patients to use if they get sicker, but it is not to be used long-term, and so far only one patient has needed it. For more information please read the recommendations on Dr. Vallings’ website: http://www.drvallings.co.nz/news-items/covid-19-vaccines
Emeritus Professor Warren Tate
I’m a strong advocate for vaccination of any family household member who is not health compromised as this provides protection for the unvaccinated, however I propose a cautious approach for all people with ME/CFS. This is because although the predictive analyses of immunologists might suggest the risk of ongoing relapse (of ME/CFS symptomatology) is small, the patient self-reporting suggests the risk is significant. For example if the person with ME/CFS experiences severe food allergies, chemical hypersensitivities, is prone to frequent debilitating relapses and has a significant compromised level of activity, then I would suspect a much higher risk in comparison to pwME/CFS who do not have these extra dimensions of the illness. In two international studies that came across my desk in regards to the Pfizer vaccine (administered here in NZ) after one dose, 10% reported severe effects on ME/CFS, 40% had mild-moderate effects and 50% had no effects. After the second dose, again 50% had no significant effects, yet nearly 30% had severe effects for at least one month, and 20% had moderate effects. Another study has reported 30% severe effects after the first dose. Anecdotally, of the three women in my university group who had the vaccine, one required hospitalisation for IV fluids after 2 weeks of being severely affected, another had two weeks of a moderate relapse and the third woman had no significant side effects. This seems to mirror the international patient reporting of the much larger groups, and made their results seem genuine to me. I believe therefore that I cannot provide a blanket recommendation for or against the vaccine, but rather believe that each individual should weigh up the decision based on their personal ME/CFS history. If pwME/CFS decide to vaccinate then I would suggest following Dr. Klimas’ antihistamine protocol.
Dr. Nancy Klimas, Nova Southeastern University
COVID kills people. It kills people with over-activated and damaged immune systems preferentially – and that is what ME/CFS is all about. So while there certainly is a risk for an ME relapse with these hyper reactive vaccines, you have to weigh the possibility of an ME relapse against the risk of death from COVID-19. For more information and for advice for people with mast cell activation syndrome visit: https://www.nova.edu/nim/To-Vaccinate-or-Not-with-MECFS.html
In conclusion from our experts
There is not a definitive answer about whether pwME/CFS should or should not get the COVID-19 vaccine. As the condition is highly individualised, so too, is the response to the vaccine. Some have no effects, some only the expected immune response, some experience improvement of symptoms, and some a worsening of symptoms or a relapse. So what is appropriate for the individual is best considered in conjunction with your GP or specialist who has access to your personal medical history.
Should you choose to vaccinate
Center for Disease Control (CDC) states that people with ME/CFS or fibromyalgia should rest for several days before and after the vaccine, as anecdotal information shows that symptoms can resurface while the immune system is activated. The CDC provide information on what to expect before and after your vaccine: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/expect/after.html
Dr. Lucinda Bateman, Bateman Horne Center states that pwME/CFS should be rested and stable prior to the vaccine, and plan on resting/relaxing for at least 72 hours afterward. Supportive care will include anything you usually do for flu symptoms, PEM, allergy flares, worsened orthostatic intolerance, etc. If anything, including a vaccine, makes you sick enough that you are unable to maintain adequate fluids and nutrition, or results in fluid and electrolyte losses (sweating, diarrhea, etc), it is always appropriate to seek IV fluids as a primary intervention.
Antihistamine Usage
Dr. Klimas suggests that before the vaccine, make sure you are taking enough antioxidants, particularly NAC or glutathione and CoQ10. Take an antihistamine before and for several days after the vaccine – the strongest one you can tolerate. Please note: that if you take the vaccine you should take the whole recommended dose, and the current vaccine Pfizer should be administered twice.
As always when dealing with medications and supplements please only do so under the direction of your General Practitioner or Medical Professional to ensure correct dosage administration and to avoid contraindications with your existing medications and personal medical history.
ANZMES is currently running a self-reporting survey of vaccination effects for pwME/CFS in NZ and will produce the results as soon as possible. We hope many will participate. If you require a survey sent by post, please let us know. https://forms.gle/BYEGhGMuaVoPVTrH6
There are some therapies which are commercially based, and they come under many names. Lightning Process is one that has been widely known. This is a psychological approach based on neurolinguistic programming, a technique that may have benefits for those who are experiencing depression or anxiety.
Claims have been made that the Lightning Process is a cure and some have said it did cure or significantly help them, but as yet no scientific trials have been done with a group selected from stringent ME/CFS or Long COVID research guidelines. It is possible responders may have conditions other than ME/CFS or Long COVID.
We are concerned by its promotion of it as a ‘cure’ for ME/CFS and Long COVID. At present this is not scientifically proven. We have received reports from those who have spent a great deal of money to try this or similar treatments who have made no improvement, have not been cured or have relapsed severely. The guilt experienced by those who are not cured can be devastating.
The following is a quote from Dr Charles Shepherd, medical advisor to the ME Association: “‘The Lightning Process’ is not a treatment that we endorse or recommend for people with ME/CFS. “Patient evidence, gathered from our members over many years, indicates that some people who have gone through the LP try to make rapid and unrealistic improvements in their physical and mental activity levels. However, this is followed by a relapse or significant worsening of symptoms. Others who have gone through the LP programme report that they have spent huge amounts of money with no obvious benefit. It may well be that there are some people with a general fatigue state, resulting from stress, emotional or psychological problems who could benefit from a ‘mind over matter’ entity and not to be confused with ME/CFS. There has been a very significant growth in biomedical research globally into M.E. in the past decade. This over-simplistic and largely psychological model of ME/CFS causation that is being put forward to patients is totally out of step with emerging scientific evidence as to the cause of ME/CFS.”
Since Dr Shepherd wrote this statement, there has been even more robust scientific research into ME/CFS as a neuro-inflammatory disease. One might do well to remember that multiple sclerosis was once seen as a kind of ‘hysteria,’ until MRI machines were able to identify the lesions associated with this disease on the myelin sheath. Research into the biomedical causes and potential treatments of ME/CFS and Long COVID is proceeding at a rapid rate and new therapies are being developed, including the possibility of treatment through using existing medications.
Along with providing support, it is the aim of ANZMES to provide sufferers of ME/CFS and Long COVID with accurate and up-to-date medical information. We encourage all patients, medical practitioners, family members or the general public to contact us with any questions you may have.
Associated Myalgic Encephalomyelitis Society of New Zealand, Inc.
Update – National Institute for Health and Care Excellence (UK) published revised guidelines on October 29, 2021. In this revision, NICE stated that the Lightning Process should not be offered as a treatment for people with ME/CFS (point 1.12.27 of the recommendations) as it could potentially cause harm. For more information visit: https://www.nice.org.uk/guidance/ng206/chapter/Recommendations