We know that any viral illness will be followed by a post-viral phase. During this time the body is theoretically in “recovery mode.” Even after a simple cold, a person can be left feeling rather drained and limp for a few days but will usually slowly recover.
In those who are diagnosed with ME/CFS, the majority will have started this illness with a viral infection, from which they never seemed to recover. When you have a viral illness, your immune system goes into “disarray” and is upsetting your whole system, seemingly fighting the virus. Gradually the fight is over and successful, and you feel recovered. But those who end up with ME/CFS have an immune system which seems to persist in the fighting mode, producing a lot of extra hormones, chemicals and many other immune system abnormalities. This is exhausting and leads to many ongoing changes and symptoms. The changes may affect the body chemistry and the metabolism further, and have far-reaching effects on the brain, muscles and other body systems.
So why should the after-effects from COVID-19 be any different? There are thousands of people around the world now being diagnosed with the condition called “Long COVID,” and immunologically and chemically, it is no different from ME/CFS – a prolonged post-viral state – often very severe.
We have to ask ourselves “Can this condition be prevented?” as there is no “quick-fix.”
Photo Credit: Martyna Reynolds
We do know however that pushing yourself hard during the recovery phase can lead to worsening symptoms and potentially to a final diagnosis of ME/CFS. After COVID-19 most people yearn to get their health back and return to a full life again. There is a temptation to return to normal as soon as possible. But there is certainly good evidence now that pushing hard mentally or physically too soon, can prolong the illness, or even cause relapse.
During the recovery phase from COVID-19, it is therefore important to take supreme care of yourself in order to minimise the risks. We know that some people are probably genetically vulnerable, and we also know that those already with a diagnosis of ME/CFS almost always will risk worsening symptoms or even serious relapse if they push too hard mentally or physically. So, we need to translate these facts to those in the recovery phase from COVID-19.
While you are recovering from COVID-19 you need to acknowledge the known facts. So,
stay home and rest while you still have symptoms (however mild)
do not indulge in hard exercise, or long work hours
go to bed early
rehabilitate very slowly and cautiously.
While this approach may not prevent a prolonged illness such as ME/CFS, you are giving yourself a good chance of regaining your pre-COVID health.
COVID-19 self-management booklet created by Our Health Hawkes Bay Whakawāteatia:
Long COVID is a condition that occurs in people with a history of probable or confirmed SARS-CoV-2 (COVID-19) infection. It usually begins 3 months from the onset of COVID-19 with symptoms that last for at least 2 months that cannot be explained by an alternative diagnosis. For some people symptoms can last months after the infection has gone. This is sometimes called post-COVID-19 syndrome or Long COVID.
Common Long COVID symptoms include:
extreme tiredness (fatigue)
shortness of breath
chest pain or tightness
problems with memory and concentration (“brain fog”)
difficulty sleeping (insomnia)
heart palpitations
dizziness
pins and needles
joint pain
depression and anxiety
tinnitus, earaches
feeling sick, diarrhoea, stomach aches, loss of appetite
a high temperature, cough, headaches, sore throat, changes to sense of smell or taste
rashes
How is Long COVID treated?
Treatment for Long COVID is similar to that of ME/CFS. It is about managing symptoms and pain.
If PEM (post-exertional malaise) is experienced, you must avoid exercise and activities that cause fatigue or increased symptoms, and conserve your energy.
Dr. Charles Shepherd provides an extensive report on Long COVID and ME/CFS. Read it here:
The Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) supports the new position paper on the Lightning Process by the World ME Alliance and does not endorse the Lightning Process for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).
The Lightning Process is a programme loosely based on concepts of neuro linguistic programming (NLP) and cognitive behaviour therapy (CBT) that is set up commercially and currently marketed as a cure for ME/CFS. This claim is not backed by scientific evidence and ANZMES shares the view of the World ME Alliance that the promotion of this programme is likely to do harm.
The National Institute for Health and Care Excellence (NICE), in the UK, revised their guidelines for the diagnosis, treatment, and management of ME/CFS stating that the lightning process should not be used as a treatment and they no longer recommend CBT. These changes reflect a shift from an outdated perspective that ME/CFS was a psychological condition and follows evidence from over 200 studies showing poor efficacy for this treatment approach.
ANZMES President, Fiona Charlton says, “there is a growing body of evidence that shows that ME is driven by physiological changes not psychological ones and telling people that they can talk themselves out of this condition, within three days, could be very harmful.
“We know that if people with ME ignore their symptoms and push themselves this can make things worse, sometimes to the point of needing hospital care.”
ANZMES agrees with the World ME Alliance who highlight in their statement that people with ME/CFS are vulnerable to exploitation due to a lack of effective treatment where programmes like the Lightning Process are just filling this void.
People living with Long COVID are also being drawn into this treatment as this is now an extension of their claims to cure ME/CFS.
Other concerns with the Lightning Process include a bias in efficacy studies, including conflicts of interest, a reported secrecy where participants are told not to speak about the programme or their symptoms and a level of shame and guilt for those who do not recover within the three days of treatment.
Charlton says, “we want to ensure that if we are endorsing a treatment for ME that robust evidence supports efficacy and this is just not the case with LP.
“What we do know is that a treatment approach that is focussed around symptom management is shown to help with the relapsing nature of ME.”
ANZMES acknowledges that neurological symptoms, such as depression and anxiety can be a part of ME/CFS and may benefit from supportive therapies but people have the right to unbiased, impartial information when being offered these treatments.
***********************
The Lightning Process was developed and trademarked by British osteopath and hypnotherapist Phil Parker.
ANZMES has been providing information, building awareness, funding research, and advocating for people with ME/CFS for the past 42 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice, globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership.
Post-infectious diseases like Myalgic Encephalomyelitis (ME) and Long COVID are more common and much more serious than most people realise. These illnesses can devastate the lives of those affected and their whānau, and there is no effective treatment or cure.
The inaugural World ME Day on 12 May 2022 aims to close this knowledge gap. Initiated by the World ME Alliance, the day is an urgent call for better recognition of ME/CFS, Myalgic Encephalomyelitis /Chronic Fatigue Syndrome, for better training of health professionals and for more research funding.
This year’s theme of World ME Day is #LearnFromME and in New Zealand the day will be marked by an online Learn From ME video event hosted by the Associated New Zealand ME Society (ANZMES). The event features presentations from New Zealand experts in biochemistry, immunology, and general medical practice. It also includes interviews with people living with ME/CFS and Long COVID. The video presentations will remain available for viewing after 12 May.
The presentations will show that despite persisting knowledge gaps, people with ME/CFS and ME/CFS experts have accumulated a wealth of knowledge that could help improve the quality of life for those affected by ME/CFS and similar diseases like Long COVID – but only if we #LearnFromME.
World ME Day: a call for better recognition of ME
ME/CFS is as common as it is disabling. It is estimated to affect 17 to 30 million people across the world with 20,000 to 45,000 in New Zealand. The majority are unable to work or study and a quarter are so seriously ill they are housebound or bedbound, a heavy personal and economic burden. Yet ME/CFS remains under-researched and poorly understood, allowing misinformation to flourish. This has resulted in ME/CFS patients being either dismissed and ignored or prescribed treatments that are unhelpful at best and harmful at worst.
A particularly little-known phenomenon is post-exertional malaise (PEM) which refers to an unusual and disproportionate increase in symptoms after minor activity. PEM is not known to occur in other illnesses but it is the cardinal feature of ME/CFS – without PEM an ME/CFS diagnosis cannot be made – and PEM is also experienced by many people with Long COVID. PEM is best managed by creating an individualised routine of rest and carefully paced activities. People with ME/CFS have a wealth of practical PEM management experience to share with those wanting to #LearnFromME.
Kate was diagnosed with ME 4 years ago after 20 plus years of health challenges triggered from a viral illness. Before this she was hardly ever sick, a school prefect and played high level sport representing New Zealand for Water Polo. In 2018 her system crashed after pushing through symptoms for too long when numerous doctors weren’t able to help. She suffered with crushing fatigue that did not improve after a full night’s sleep and had to give up work, sports and her social life. She was mostly confined to her home, except for dropping off and picking up her boy from daycare/school and other activities. She also experienced constant body pain, fluctuating headaches, neurological problems resulting in impaired memory and an inability to concentrate and Postural Orthostatic Tachycardia Syndrome (POTS), a dysfunction in the autonomic nervous system. Any physical, mental, or emotional effort would cause worsening of her symptoms and she had to learn to work within a very small energy envelope. Four years on, Kate has made what is known as significant progress in the ME community, with a reduction in symptoms enough that she can work a small number of hours each week. She can attend more activities with her son, however her dreams of dancing and playing masters level competitive sports are not fulfilled and she is accepting that she may never reach these and other dreams she has.
World ME Day: a call for better training of health professionals
The key roles of PEM and pacing are reflected in recent updates to clinical guidance around the world. On World ME Day healthcare professionals are encouraged to familiarise themselves with one of these. In New Zealand the regional DHB HealthPathways websites provide up to date clinical advice. Internationally the National Institute for Health and Care Excellence (NICE) in the UK, and the CDC (Centers for Disease Control and Prevention) and Mayo Clinic Proceedings in the US, are excellent resources. Continuing medical education credits are available for New Zealand health professionals who want to #LearnFromME.
GP Cathy Stephenson states “ME affects 10s of 1000s of kiwis and their families every day, yet evidence-based management and support is almost impossible to access. As a health sector, we need to upskill rapidly – Long COVID appears to be remarkably similar to ME, and when the predicted tsunami of it reaches our shores, we will struggle to cope unless we act now.”
“In the future it would be wonderful to have specialist centres set up to provide the very best care to patients with ME and Long COVID, but for now my hope is that every health provider in primary care is able to offer a safe, affirming, evidence based approach to managing this debilitating condition.”
“If there’s one thing to impress upon health providers when it comes to the management of ME/CFS, its Pacing. Above all else. Pacing.”
World ME Day: a call for more research funding into ME and other post-infectious diseases
The coronavirus pandemic has impacted the ME/CFS community in two ways. More people with ME/CFS are more seriously ill after their already poor health and quality of life deteriorated further following a COVID-19 infection. And more people are being diagnosed with ME/CFS as increasing numbers of Long COVID patients meet diagnostic criteria for ME/CFS.
It remains unclear if post-viral ME/CFS and post-viral Long COVID are one and the same disease or two very similar ones. What is clear is that both groups desperately need effective treatments and ultimately a cure. Much more funding is needed for rigorous biomedical research to build on what we can already #LearnFromME.
Emeritus Professor Warren Tate and his research team at Otago University have contributed substantially to our improved understanding of post-viral illness.
Tate says “It was exciting to find molecular signatures in the immune cells of ME/CFS patients associated with dysfunctional energy production and showing instability in the epigenetic code that controls precise production of all our proteins, giving a clear indication of the biological basis for the illness.”
“Long COVID and ME/CFS have very similar molecular signatures for proteins connected to immune dysregulation, inflammation and energy production.“
“The fact that ME/CFS is so functionally debilitating, and is life-long in most cases, puts huge social and financial burdens on those affected, their families and their communities, and blunts the potential of highly productive people to contribute value to our society.”
World leading researchers for ME/CFS and Long COVID here in New Zealand are hampered by inadequate funding. With funding, these researchers can contribute to improving the quality of life for people with ME/CFS: Emeritus Professor Warren Tate, Biochemist, University of Otago; Dr Lynette Hodges, Exercise Physiologist, Massey University; Dr Anna Brooks, Immunologist, University of Auckland.
May 12 is World ME Day. This year, the Learn From ME global campaign acknowledges that people with ME/CFS are experts of their own illness experience. They have a lot to offer those experiencing Long COVID through insights, treatment plans that work and understanding of what it is like to live with a chronic illness.
What can the Long COVID community learn from ME/CFS?
That post-viral syndromes are real. Some people recover, others don’t and this is determined by the unique physiological makeup of each individual. They can learn to pace themselves, to not give up, and to have hope with new research being released. They can learn to advocate for themselves and they will learn and know that the ME/CFS community supports them.
Resting is key to being able to achieve activities. Pacing is vital for sustaining periods of activity. Pacing is a common management tool for people with ME/CFS. When you apply pacing to your life, you are taking control of how you spend your time – finely balancing activity with rest to prevent overexertion. For people with ME/CFS overexertion can result in what is known as post-exertional malaise (PEM) – whereby a relapse of symptoms can cause the person to be bed bound for days unable to care for themselves, or they experience an exacerbation of core symptoms for several weeks. This can happen to people with ME/CFS not only with physical activity but mental/cognitive activity too.
“I learned how to pace the hard way.” Says Jane, a person with ME/CFS. “After repeatedly over-doing it by trying to get things done on one of my good days and then crashing and being bed bound for days after, I slowly learned how to pace my activities. Now I will put a load of washing on and then rest. I’ll peg the washing out and then rest. I can then start on the vacuuming. The key is to learn that I can vacuum one room one day and another room another day. I don’t have to get it all done at once. Balancing between activity and rest means I can sustain activity for longer without causing a relapse of my symptoms.”
Such post-exertional malaise and inability to maintain activity is said to be as a result of malfunctions in the energy production system. Research by Dr. Lynette Hodges from Massey University who has studied PEM extensively shows significant differences in exertion capabilities of people with ME/CFS when compared to healthy controls.
Kathy says “I learned that what I can achieve on one day, I may not be able to achieve on another day. I usually have to spread activity out across the week, it means having an appointment on a Monday and resting on a Tuesday. I have to recover from the exertion of getting showered, dressed, fed, before driving to my appointment, and then the cognitive exertion required to function at that appointment, before getting myself back home. I used to go to the gym 7 days a week, sometimes twice a day, and work full-time, travel, and play sports on the weekend. I lived a full life, now I’m lucky if I can manage to do one thing in a week!”
Photo Credit: Martyna Reynolds
Recently someone experiencing a COVID-19 infection, talked to her ME/CFS friend “I had to rest for an hour after pegging the washing out. It made me think of you, I don’t know how you deal with this every day, year in year out.”
Edith says: “I’ve learned to not give up. I have hope that with new research being released we will no longer face stigma, that everyone will know this disease is real, and the research proves this.”
By sharing their experiences, it is hoped that the general public, friends, family/whānau, and medical professionals and institutions gain valuable insights about this often maligned condition. For decades there have been misconceptions about this disease. Despite the World Health Organisation classifying it as a neurological disorder in 1969, and adding it as a “post-viral syndrome” in 2019, many health professionals still follow the misguided and unfounded school of thought that it is psychological or psychiatric in nature.
The growing body of biomedical research from around the world and here in New Zealand demonstrates otherwise. Emeritus Professor Warren Tate has identified a biological basis for ME/CFS symptoms. He has shown a dysfunction in the mitochondria (energy-making function of the cell) in people with ME/CFS and disturbed widespread physiology, highlighting the complex chronic nature of this illness. He has also recently submitted a paper regarding the biological processes that facilitate relapse and sustain ME/CFS.
The ME/CFS community has had to be vocal, has had to stand up to misinformation, has had to demand funding for research, and has had to beg for ministry support.
Recently retired, general practitioner, and long-time advocate for people with ME/CFS, Dr. Ros Vallings says “It is so important to get a correct diagnosis according to specific recognised criteria. That way a treatment plan can be established which is most likely to help manage symptoms.” ME/CFS is an umbrella term for a cluster of debilitating symptoms that result from malfunctions in multiple bodily systems. Despite the person often appearing ‘well’ these debilitating symptoms include but are not limited to: incapacitating exhaustion, post-exertional malaise, pain, sleep disturbances, cognitive and gastro-intestinal issues, and orthostatic intolerance (severe light-headedness when standing).[1]
In NZ there are at least 25,000 people living with ME/CFS – that’s approximately 1 in every 250 adults and 1 in every 134 youth.[2] It commonly has acute onset (occurs suddenly) after a viral illness (e.g. Epstein Barr/Mononucleosis and SARS-CoV)[3]. The illness affects all genders, races and ethnicities. It affects children, those at university still studying, those just entering the workforce, mums and dads juggling home and work and people at the peak of their careers, right up to the elderly who already have other struggles. Some will recover after some months or years, but those who are still sick two years after onset are likely to suffer this illness for the rest of their lives. Dr Sarah Dalziel ANZMES medical advisor says “There are around 3,000 young people in New Zealand with ME/CFS and life can change dramatically for them when they get this illness. “Adolescents with ME/CFS identify that remaining engaged in education and therefore the ability to pursue future aspirations is crucially important. This requires a lot of support and education for teachers and parents to help children design an achievable plan for schooling.”
With omicron rife in New Zealand, yet another post-viral syndrome is looming. Of all COVID-19 cases, an estimated 10-30% may develop what is commonly referred to as Long COVID.[5] Many of these will go on to receive an ME/CFS diagnosis too. With over 1 million COVID-19 cases in NZ, that means roughly 100,000-300,000 people could become so ill that they can no longer work, attend school, and for some it will mean a lifetime being bedbound unable to care for themselves, or housebound, unable to maintain consistent activity. This will have huge economic, political, and psychosocial impacts. The government has largely ignored the high percentage of people with ME/CFS in New Zealand who are unable to work or finish school because of their illness. They will not be able to ignore the tide of illness that is threatening to reach our shores very soon. Post-viral syndromes are catastrophic not only in the personal lives of those who are ill, but to their families, community, and have far-reaching economic impacts, it will over-burden our healthcare systems, and may result in more people having to rely on government benefits to survive. It is time to wake up. It is time to invest money in research. It is time to #LearnFromME.
May 12 marks the international Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Awareness Day, on Florence Nightingale’s birthday (as it is thought she developed ME/CFS after an infection contracted during the Crimean war). Each year on this day ANZMES (the Associated New Zealand ME Society) seeks to provide education and build awareness, as well as advocate for and support those with ME/CFS and their families. This year, the theme for World ME Day is Learn from ME. In conjunction with the World ME Alliance, ANZMES seeks to demonstrate the volume of knowledge that the ME/CFS community can provide.
The Learn From ME Event on May 12, hosted on the ANZMES website provides presentations from Professor Warren Tate, Dr. Anna Brooks, Dr. Rosamund Vallings, and includes two interviews of the lived experience.Resources are available for patients, carers, teachers and health professionals through the Associated New Zealand ME Society (ANZMES) at www.anzmes.org.nz.
The World ME Alliance, a collaborative of organisations from across the globe, is launching World ME Day on 12th May this year. This new initiative aims to bring together organisations and unify efforts to raise awareness and campaign together on Myalgic Encephalomyelitis (ME). Through collective action, we will step closer to our goal of a world without ME.
World ME Day will build on the incredible efforts of advocates around events, such as ME Awareness Week and Chronic Immunological and Neurological Diseases (CIND) Awareness Day. By focusing on a single day and collaborating across many organisations, we aim to maximise our collective power.
The theme for the first year of World ME Day is #LearnFromME.
ME is a global health crisis – up to 30 million people are living with this disease worldwide, and when we take into account the effect on families, carers and friends too, the impact of this disease cannot be overstated.
But there is much to be learnt from this disease – from the willpower and determination of those living with it, to the incredible advocates working towards change, to an understanding that the most meaningful change will comes from high-quality research.
We want to use World ME Day to reach out to health professionals on a personal basis, build understanding of ME and take another step towards a world that understands ME.
Key facts for health professionals
People with ME have a lower average quality of life than all other diseases they have been compared to, including diabetes, cancers and heart disease.
The government mandate stipulates that certain industries require vaccination in order to retain employment. Although we have advised MoH that this is not as simple for those people with ME/CFS (pwME) who are affected by this Order, we have not been able to change their decision through our advocacy efforts.
For pwME who are not employed in the mandated industries, there will still be barriers if they choose to remain unvaccinated due to the introduction of vaccine certificates/passports. However the decision to vaccinate or not vaccinate remains a personal choice.
ANZMES provided MoH with a detailed argument in favour of MoH allowing physician discretion on a patient-by-patient basis as to whether a medical exemption is warranted. We have not received a response to our advocacy from MoH to date. The argument stipulated that only the physician and the patient can truly know, based on the patient’s personal medical history, whether a risk of adverse reaction is sufficient enough to warrant a medical exemption.
This was based on Professor Warren Tate’s advice that people with ME/CFS who often experience severe food allergies, chemical hypersensitivities, are prone to frequent debilitating relapses and have a significant compromised level of activity, may be at a higher risk to adverse side effects to vaccination in comparison to people with ME/CFS who do not have these extra dimensions of the illness.
For pwME who do not have these extra dimensions of the illness, ANZMES released an information sheet regarding COVID-19 vaccinations for pwME, which included expert advice from New Zealand and internationally. The recommendations provided by these experts were that contracting COVID-19 poses a greater risk to health than the side effects of the vaccination. However for a small percentage of pwME, the potential adverse reactions may seem to outweigh the risk of contracting the virus. This is because there is potential for a relapse of ME/CFS symptoms. And because household members can provide a level of protection to unvaccinated members if they themselves are vaccinated. [https://anzmes.org.nz/experts-talk-covid-19-vaccine-for-people-with-me-cfs/]
The preliminary findings of the self-reporting survey ANZMES conducted with the ME/CFS and Long COVID community suggests that the reactions to the vaccine have been as varied as the symptomatology of ME/CFS itself. For some there was no adverse reaction. Some improved. For others, only the normally expected immune response was experienced. Whereas for a significant smaller percentage there was a considerable relapse. There does not seem to be a pattern as to who fares well and who experiences a relapse. Although the survey findings suggest that the more disabling the ME/CFS symptoms, the more prone to a relapse after vaccination, relapse can occur at any functional capacity state for pwME. However, it is also likely that no adverse reactions, or only temporary reactions are experienced. This shows how highly individualised vaccine reactions are, just as is the case for the symptomatology of ME/CFS. [https://anzmes.org.nz/anzmes-preliminary-survey-findings/]
ANZMES also petitioned for a fractionated dosing trial at the request of the community. Although this trial will not go ahead, IMAC are investigating the possibility of lower dosing. However, as trials have not been done, MoH advises that lower doses will not be considered sufficient for protection and therefore someone who receives a fractionated dose would not be eligible for a vaccination certificate/passport. Research into the efficacy of lower doses as protection against COVID-19 would need to be conducted in order for this to change.
It was reported by RNZ as a quote from a MoH spokesperson, that there is not sufficient evidence to suggest that lower dosing will mitigate adverse reactions to the vaccine. It is correct that no trials have been conducted into reactions to lower dosing for pwME. However, in studies that have been conducted into fractionated dosing, reduced doses appear to reduce reactogenicity (adverse side effects).
ANZMES does not provide medical advice or opinions as an organisation, the information provided above is a summary of expert advice and government information. This is so that the ME/CFS community can be informed of all sides of the situation, and can therefore make decisions based on their own individual circumstances. As always, this should be done in conjunction with the individual’s usual medical professional(s).
At the request of the ME/CFS community, ANZMES has issued a survey relating to reactions experienced by the community to the COVID-19 Pfizer BioNTech vaccine. ANZMES also sought to ascertain prevalence of Long COVID and COVID-19 infection in the community. The opportunity was also utilised for respondents to express interest in participating in a potential fractionated dosing trial.
This report contains preliminary findings for responses received from 21st October 2021 to 10th November 2021. This survey is still open to capture experiences after these dates, as vaccination decisions are ongoing.
Please note that this survey is classed as a self-report questionnaire which seeks to ascertain the subjective experience of people with ME/CFS and co-morbid conditions. The information collected is therefore anecdotal data. No clinical research has been conducted.
Respondents
395 respondents identify with an ME/CFS diagnosis
144 with Fibromyalgia (some overlap with ME/CFS)
19 with COVID-19
5 diagnosed with, and 32 suspect, Long COVID
The majority of respondents have a clinical diagnosis of ME, with 25 self-diagnosed. Most are unsure as to which diagnostic criteria for ME was used.
Some questions have less respondents, therefore numbers are indicated in the relevant sections.
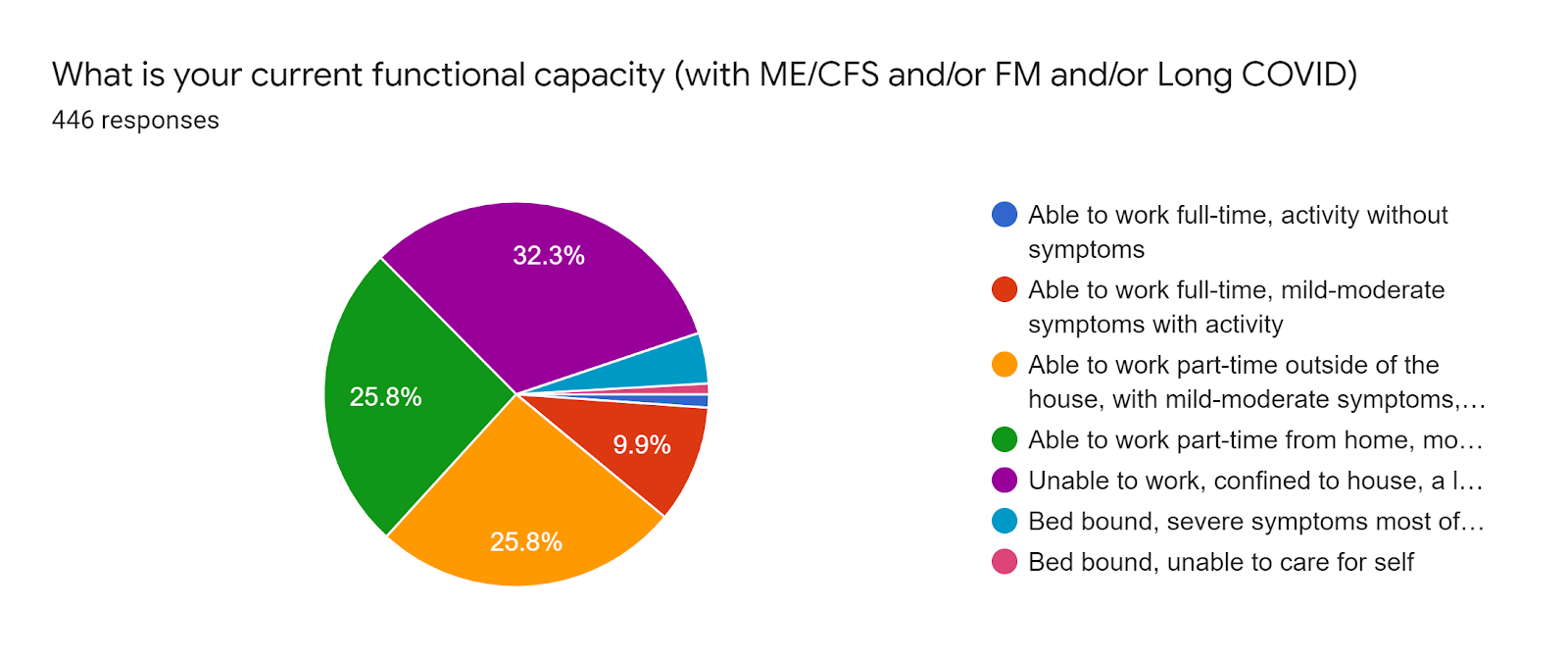
Functional capacity (pre-vaccination)
32.3% (144 individuals) are unable to work, confined to their home with a lot of rest required.
25.8% (115) are able to work part-time at home.
25.5* (115) are able to work part-time outside of the house.
9.9% (44) are able to work full-time with mild-moderate symptoms with activity. 1.1% (5) are able to work full-time without symptoms. * These respondents were mostly COVID-19 infection or Long COVID respondents without ME/CFS.
4.3% (19) are bedbound most of the time.
0.9% (4) are bedbound and unable to care for themselves.
Vaccination rates
The majority of respondents have had two doses of the Pfizer vaccination.
64.5% (296) two doses.
16.1& (74) single dose.
19.2% (88) have not been vaccinated.
Of the 296 with two doses, the duration between doses was 6 weeks or more for 166 individuals and 3 weeks for 130.
Pattern for capacity and reaction
These findings suggest that the more disabling the ME/CFS symptoms, the more prone to a relapse after vaccination but that relapse can occur at any functional capacity state for pwME. This was analysed when there were 241 responses.
Temporarily worsened
Improved
No change
Worsened into relapse
Worsened beyond illness
Not vaccinated
No answer
Part-time work home
22
8
7
9
1
14
2
Part-time outside house
22
3
17
14
0
12
2
Full-time work mild-mod with activity ME FM Long COVID/COVID
3 2 0
0 0 2
4 1 3
3 1 0
0 0 0
2 0 1
2 0 5
Unable to work, confined to house
23
6 3 temp
15
18
7
8
7
Bedbound mostly
2
0
0
3
0
1
1
Bedbound unable to care for self
0
0
0
1
0
1
1
Overall ME
72
20
43
48
8
30
20
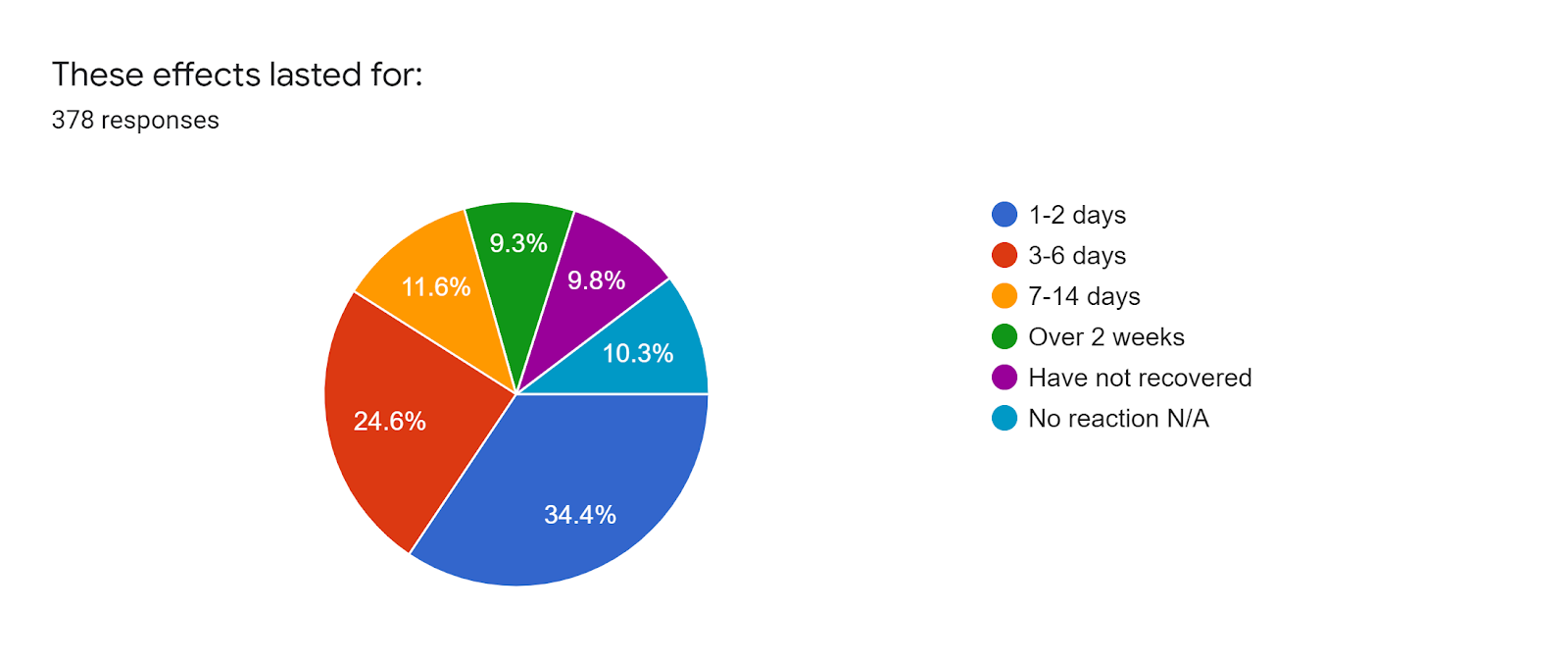
First dose vaccination reaction and duration
There were 39 individuals who did not experience any symptoms. For those who did experience reactions to the first dose of the vaccine, these were consistent with the expected normal immune response, e.g.:
sore at injection site (300)
tired/fatigued (219)
Headache (142)
nausea/gastrointestinal issues (62)
fever/chills (56)
Swollen lymph nodes (46)
Sleep issues/insomnia (44)
5 people experienced heart palpitations and/or anxiety 3 people experienced skin sensitivity and/or allergy flares, with 2 people experiencing brain fog/cognitive issues.
For most people (130) these symptoms lasted 1-2 days.
For 93 individuals it lasted 3-6 days.
44 experienced symptoms for 7-14 days.
35 for over 2 weeks.
37 have not recovered.
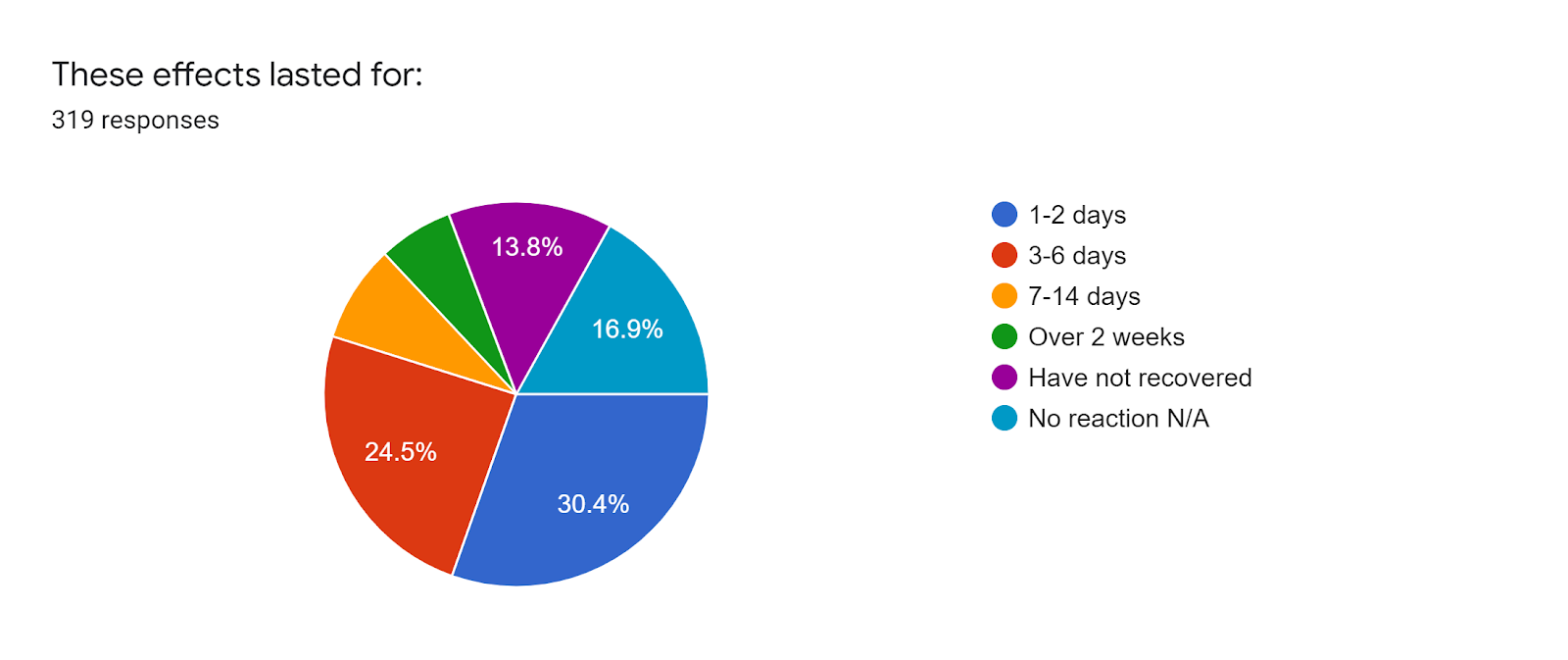
Second dose reaction and duration
As has been reported by the general public, the findings from this survey suggest that pwME also experienced more adverse reactions to the second dose of the Pfizer vaccine. However there were 54 individuals who did not experience any symptoms.
For 97 individuals these symptoms lasted 1-2 days.
For 78 individuals it lasted 3-6 days.
26 experienced symptoms for 7-14 days.
20 for over 2 weeks.
44 have not recovered.
Vaccine effect on state of illness/wellness for 359 respondents
137 (38.1%) experienced no change/stay the same
118 (32.9%) temporarily worsened but have returned to baseline
71 (19.8%) worsened and not returned to baseline – relapsed
22 (6.1%) improved
11 (3.1%) worsened beyond anything experienced in illness to date – severe relapse
289 respondents did not have any new symptoms that they could attribute to the vaccine.
52 stated that they had new symptoms that they could attribute to the vaccine. These symptoms tended to be over-activation of the immune response, e.g. sore throat, swollen neck glands, allergy reactions. Of these 52 – 4 individuals have gastrointestinal issues, 2 experienced more fatigue whilst 1 indicated improved energy.
Clinical care
From 383 responses 314 (82%) were not offered clinical care during vaccination, 15 (3.9%) were offered clinical care, 19 (5%) were unsure. 25 people asked for specific clinical care during the vaccination process. Of those offered clinical care the options were 30 minute observation rather than the normal 15, separate areas with direct nurse observation. Others were advised by their GPs to rest and take antihistamines pre- and post-vaccination.
Caregiving requirements
From 353 respondents 50 require ongoing caregiving for their ME/CFS and/or FM and 70 required care after vaccination. 244 people do not require caregiving before and 230 after.
Fractionated dosing interest
If fractionated / lower dosing had been an option, of 115 responses 48 stated they would have considered it, 23 said they would not consider it and 44 were unsure.
Of 88 responses for those reluctant to have the vaccine, 57 would consider lower dosing options, 10 would not, and 21 were unsure.
Of 124 responses to indicate interest in participation in a potential trial into fractionated dosing, 61 responded that they are interested, 31 may be interested, and 32 are not.
Antihistamine usage
Of 115 responses 45 did not take any pre- or post-vaccination, 70 did.
Reasons for not being vaccinated
Of 1Anxiety/worry/fear about potential adverse reactions, previous adverse reactions to other vaccines, concern about the safety of the vaccine, high ME/CFS symptomatology, chemical sensitivities/MCS/MCAS, not currently well enough to risk adverse reactions.
COVID-19 / Long COVID
19 respondents have been diagnosed with SARS-CoV-2 (COVID-19) infection.
169 respondents have had COVID-19 tests.
5 people have been diagnosed by a medical professional with Long COVID.
32 people suspected they have Long COVID after a viral infection due to ongoing or lingering classic COVID-19 symptoms and having been connected to a location of interest, an overseas hot zone of infection, or have remained unwell after experiencing a viral infection that has not been confirmed as COVID but has the same symptoms.
One of the primary objectives of ANZMES (Associated New Zealand Myalgic Encephalomyelitis Society) is to further the cause of ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome) through the promotion and funding of research into the disease. The global COVID-19 (SARS-CoV-2) pandemic has changed the way the world operates, interacts, and deals with new viruses. Yet the notion of post-viral syndromes is nothing new. People with ME/CFS who remain in a ‘state of dis-ease’ after glandular fever (Epstein Barr/mononucleosis) will attest to this. Likewise, an estimated 30% of people who had COVID-19 infections have not returned to their pre-illness state of health. This rising problem recognised by health professionals worldwide was initially coined as Long-hauler then Long COVID. The World Health Organisation (WHO) recently released a Clinical Case Definition, further acknowledging the problem faced by millions globally. The current WHO case definition states that:
“Post COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include fatigue, shortness of breath, cognitive dysfunction but also others which generally have an impact on everyday functioning. Symptoms may be new onset, following initial recovery from an acute COVID-19 episode, or persist from the initial illness. Symptoms may also fluctuate or relapse over time. A separate definition may be applicable for children.”
As previously highlighted in the ANZMES May 2021 press release for ME Awareness Day, there are striking similarities between the symptoms experienced by people with Long COVID and the symptoms experienced by people with ME/CFS. Besides the three mentioned in the WHO definition above, there are also flu-like symptoms (fevers/chills, muscle/joint aches/pains, headache, swollen lymph nodes) and gastrointestinal issues. These symptoms seem common in people experiencing post-viral syndromes, and yet people with ME/CFS and Long COVID experience additional symptoms unique to their conditions. For example, many with ME/CFS also endure autonomic dysfunction (dysautonomia, orthostatic intolerance), neuroendocrine malfunctions (cold extremities, intolerance to extreme heat/cold), immune over-activation (sensory, chemical, and environmental sensitivities) and other symptoms related to neuroinflammation and metabolic dysfunction. Those with Long COVID can be prone to depression or anxiety as a direct result of being chronically ill and may also have organ damage caused by the SARS-CoV-2 virus. Science and medicine still have much to learn about both conditions. For instance, why do some people contract COVID-19 and recover within a few weeks whilst others develop a persisting post-viral condition? Many of those infected in the first wave of the pandemic remained unwell more than 19 months later. Is the virus still present and active in the body or has the immune system gone haywire – stuck in a loop of search and destroy? Why does the immune system malfunction? What clues can the molecular structure of people with ME/CFS provide that may answer these questions for those with Long COVID? How can understanding Long COVID help people with ME/CFS?
These questions and more are the focus of a new study currently underway in New Zealand by co-investigators Dr. Anna Brooks, Senior Lecturer (School of Biological Sciences, Faculty of Science, University of Auckland) and Emeritus Professor Warren Tate (Department of Biochemistry, University of Otago) with Dr. Rosamund Vallings from Howick Health & Medical Centre as the key clinical investigator. ANZMES is pleased to provide partial funding for this research. Seed funding has also been awarded by Dr. Brooks’ department, Faculty, and the Maurice Wilkins Centre, a Centre for Research Excellence. However, most of the funding has been obtained via crowdfunding hosted by the University of Auckland Foundation. This funding avenue is still open and accepting donations: http://bit.ly/3AuTiYN
Dr. Anna Brooks Photo credit: University of Auckland
Emeritus Professor Warren Tate Photo credit: University of Otago
Dr. Brooks states “There is an urgent need to improve our understanding of the underlying biomedical mechanisms and immune dysfunction associated with Long COVID and other post-viral diseases. Already research is beginning to reveal the similarities between certain lingering symptoms following COVID-19 illness and ME/CFS. Patient groups are now strongly advocating for biomedical research on Long COVID to be collaborative, multidisciplinary and importantly, draw on the experience of those who have been investigating biomedical causes and mechanisms of ME/CFS.”
The experience Dr. Brooks refers to is that of Prof. Tate, winner of the Rutherford medal in 2010, who has been investigating ME/CFS since 2012, and has identified molecular signatures of ME/CFS. As co-investigators for this new study, Dr. Brooks and her team are conducting immunological studies and Prof. Tate and his team are performing molecular studies of Long COVID and its relationship to ME/CFS. Prof. Tate aims to perform molecular analyses on a subgroup of this study in addition to providing samples from his ME/CFS patient group for analysis of immunological status before and after vaccination. In addition to being an experienced cellular immunologist, Dr. Brooks is also Director of Auckland Cytometry, the core facility which houses the leading-edge technologies necessary to perform these critical analyses.
How will this research benefit the ME/CFS community? Since a certain percentage of people with Long COVID symptoms also fit the diagnostic criteria for ME/CFS and many go on to receive this diagnosis as well, the samples analysed as part of this study will be beneficial in tracking early onset ME/CFS in comparison to Long COVID. It is hoped that the researchers will be able to identify key markers of immune dysfunction, especially as a percentage of samples will be obtained at very early stages of disease. This investigation into the unique immune signature of ME/CFS and Long COVID has the potential to unveil a biomarker specific to these conditions. As Dr. Brooks’ core expertise is with advanced flow cytometry, this research will screen for over 100 immune cell biomarkers which to date supersedes any previously screened for in ME/CFS research. “This will be a world first.” states Dr. Brooks.
ANZMES is proud to play a part in this exciting new research endeavour into ME/CFS and Long COVID and will continue to update the community with news as the study progresses. As always, ANZMES welcomes donations which enable continual contributions towards vital and potentially life-changing research: www.anzmes.org.nz.
We have received many queries from our membership about COVID-19 Pfizer vaccination effects for people with ME/CFS in New Zealand.
To answer these questions confidently and comprehensively we decided to create a self-report survey which asks you about your experience with the vaccine. Whether you’ve experienced mild, moderate, severe, or no effects, we would like to know. If you have chosen not to get the vaccination we would still like you to respond. If you are too unwell to fill out the survey yourself, you can ask someone else to fill it out on your behalf.
This survey also features questions regarding experiences and diagnoses of Long COVID as we seek to understand the prevalence and similarities to ME/CFS.
We hope many will participate in this vital research survey. If you require a survey sent by post, please let us know.