The Aotearoa New Zealand Myalgic Encephalomyelitis Society (ANZMES) has released a call to action urging healthcare providers to advocate for equitable policies and compassionate care for patients living with chronic illnesses such as Myalgic Encephalomyelitis (ME/CFS), Long COVID, and other complex conditions.
The NZ Doctor Rata Aotearoa published the opinion piece by ANZMES president, Fiona Charlton, on Tuesday 29th April 2025, with content available exclusively to subscribers.
A poignant example of the challenges faced by vulnerable patients is the case of Rhiannon Purves, who has ME/CFS and dysautonomia. During a prolonged hospital stay, she was subjected to New Zealand’s hospital benefit reduction policy, which drastically reduced her weekly benefit to $56.58, leaving her unable to afford critical living expenses.
“This policy imposes severe financial and emotional hardships on hospitalised individuals, often compounding their medical challenges,” says Fiona Charlton, President of ANZMES. “Doctors have an essential role in advocating for their patients by championing policy change, assisting with bureaucratic processes, and addressing systemic inequities.”
The pressing need for action extends beyond policy reform. Patients with ME/CFS and Long COVID frequently encounter systemic care gaps, including misdiagnoses and outdated treatment protocols that worsen their conditions. ANZMES highlights practical steps for healthcare providers, including:
– Writing detailed advocacy reports to ensure patients receive necessary care and support.
– Participating in Continuing Medical Education (CME) training on ME/CFS, available through ANZMES’s Know M.E. Series and My Health Hub.
– Supporting initiatives like ANZMES’s petition to abolish benefit cuts after 13 weeks of hospitalisation.
“Doctors are not only caregivers but also key advocates for systemic change,” says Charlton. “By supporting vulnerable patients, healthcare providers can drive policies that prioritize fairness, inclusivity, and improved care outcomes.”
ANZMES invites healthcare professionals and the broader community to join their efforts by signing the petition on Action Station and engaging with educational resources to better understand ME/CFS and Long COVID.
Together, we can reimagine a healthcare system where no patient is left behind.
ANZMES Highlights Lessons from the COVID-19 Pandemic in Submission to Royal Commission
ANZMES (The Associated New Zealand Myalgic Encephalomyelitis Society) has made a detailed submission to the Royal Commission of Inquiry into COVID-19 Lessons Learned, underscoring the need for equitable and inclusive public health measures in future pandemic responses.
Drawing on over 40 years of expertise supporting individuals with ME/CFS, ANZMES’ submission reflects the unique experiences and challenges faced by vulnerable populations during the pandemic. It emphasises actionable lessons to strengthen public health planning, safeguard chronic illness communities, and foster trust in healthcare systems.
Key insights from the submission include:
Addressing systemic gaps in vaccine safety protocols, adverse reaction reporting, and mandates, with tailored guidance for vulnerable populations like those with ME/CFS and post viral conditions.
Reinforcing the importance of equitable lockdown measures, including flexible service delivery and targeted mental health support for vulnerable populations, including chronically ill individuals.
Promoting inclusive design of testing, tracing, and public health technologies to ensure accessibility for populations with cognitive impairments and limited mobility.
Advocating for ongoing support for post-viral illnesses through the establishment of a Centre of Excellence, fostering research, education, and patient-centered care.
“The COVID-19 pandemic revealed critical gaps in the recognition and support of individuals with chronic illnesses, like ME/CFS and long COVID,” said Fiona Charlton, President of ANZMES. “Our submission calls for proactive and inclusive strategies to ensure that these populations are no longer overlooked in future public health crises.”
ANZMES’s submission reflects a steadfast commitment to advocating for systemic reform and fostering collaboration with policymakers, healthcare providers, and communities to build a resilient and equitable healthcare system.
Ends.
Understanding ME/CFS and long COVID Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a long-term, multi-systemic illness affecting the nervous, endocrine, autonomic, cardiovascular, and immune systems. It is often triggered by a viral illness and involves overwhelming fatigue and other symptoms that range in severity. Patients experience severe fatigue, post-exertional malaise (PEM), unrefreshing sleep, cognitive impairment, and orthostatic intolerance (to list a few). With over 100-200+ potential symptoms, the condition’s impact can vary greatly, making diagnosis and management highly individualised. Roughly 25% of all ME/CFS cases are categorised as mild, 50% as moderate-severe and 25% as very severe.
Long COVID (LC) is characterised by persistent, unexplained symptoms following infection with COVID-19 (SARS-CoV-2) lasting more than 12 weeks and not explained by an alternative diagnosis. Both conditions share symptoms such as extreme fatigue, cognitive dysfunction, and post-exertional symptom exacerbation (PESE), with up to 50% of long COVID cases fitting the diagnostic criteria for ME/CFS.
COVID developing to ME/CFS
Using data from a long COVID research initiative run by the US National Institutes of Health (NIH), the incidence of ME/CFS is now considered 15 times higher than pre-pandemic levels, and that people with a history of COVID are almost eight times as likely to develop the chronic condition.
Post-Exertional Malaise (PEM)
Post-Exertional Malaise (PEM), also referred to as post-exertional symptom exacerbation (PESE) in the context of long COVID, is a debilitating response to normal, every-day activities in people with ME/CFS. For individuals with severe-very severe ME/CFS or LC, this can be triggered by sensory overload, such as exposure to light or even simple conversations. Repeated episodes of PEM can exacerbate these already severe symptoms, and even minimal exertion can lead to significant setbacks for the patient’s health and wellbeing.
About ANZMES The Associated New Zealand ME Society is the National Advisory on ME/CFS. Established in 1980, ANZMES has been at the forefront of research, representation, and education for ME/CFS in Aotearoa/New Zealand. The organisation’s expertise comes from its reputable medical team of advisors, which includes a world renowned expert and MNZM recipient, a fellow of the Royal NZ College of General Practitioners (RNZCGP) and a network of academic researchers, clinicians, and representatives from the ME community.
The organisation is a registered provider of continuing medical education with the Royal New Zealand College of General Practitioners (RNZCGP) and is dedicated to improving the lives of those affected by ME/CFS, long COVID, and associated conditions.
ANZMES is a founding member of the World ME Alliance, and a member of the Neurological Alliance NZ, long COVID Alliance, Carer’s Alliance, Disabled Person’s Assembly (DPA) and Access Matters.
The organisation’s vision is to live in a world where Myalgic Encephalomyelitis (ME)/ Chronic Fatigue Syndrome (CFS), long COVID (and associated conditions) are recognised, supported, diagnosed early, treated effectively, and cured.
The vision focuses the organisation’s mission as the trusted leader to fund and generate robust Aotearoa research, represent the global voice, and educate through best practice to improve outcomes.
The vision and mission drive the organisation’s purpose as the leading National Advisory to produce and deliver quality, reputable, authoritative, evidence-based information, data, research, and education. We represent the needs of the community to ensure best outcomes are the primary focus of healthcare, legislation, and services that affect people living with ME, long COVID, fibromyalgia, and dysautonomia.
The New Zealand Royal Commission has opened an inquiry into the COVID-19 pandemic, seeking to gather information from New Zealanders (individuals and organisations) for their “COVID-19 Lessons Learned” Inquiry to ensure that Aotearoa/New Zealand is as prepared as possible for future pandemics.
Question 1: Looking back – what would you like the Inquiry to know about your experiences of the pandemic?
Question 2: Moving forward – what lessons should we learn from your experiences so we can be as prepared as possible for a future pandemic?
ANZMES has made a submission in consultation with the Aotearoa/NZ ME/CFS organisations as follows:
As the National Advisory on Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome (ME/CFS), we appreciate the opportunity to provide feedback for the inquiry into the pandemic response, from the perspective of people living with ME/CFS. ANZMES and the regional Aotearoa/New Zealand ME/CFS organisations have been at the forefront of supporting individuals with both ME/CFS and long COVID and advocating for their rights and needs, especially during public health crises, such as the recent pandemic. We provide the following feedback and experiences at the request of our members and the regional organisations.
Question 1: Looking back – what would you like the Inquiry to know about your experiences of the pandemic?
ME/CFS is a debilitating chronic illness characterised by post-exertional malaise (an exacerbation of symptoms after minimal exertion), and a range of other symptoms that significantly impact daily functioning, such as pain, cognitive impairment, and orthostatic intolerance (blood pressure and volume dysregulation). There has been a significant increase in cases of ME with a shift to COVID-19 being the main trigger. There are estimated to be 65 million cases of long COVID worldwide and at least half of these meet the criteria for an ME/CFS diagnosis.1 ME/CFS and long COVID are both post-viral illnesses that benefit from a similar approach to support and management. The National Institute for Health and Care Excellence (NICE) in the United Kingdom acknowledges that the physical symptoms of ME/CFS can be as disabling as those in multiple sclerosis, systemic lupus erythematosus, rheumatoid arthritis, congestive heart failure and other chronic conditions.2 Other research shows that people with ME/CFS score lower overall on health-related quality of life tests than most other chronic conditions. Throughout the pandemic, individuals with ME/CFS have faced unique challenges and vulnerabilities that have often been overlooked in the broader public health response. We highlight the following key areas of concern:
Lack of nuanced response for prevention and protection: One of the key shortcomings in the pandemic response was a lack of nuanced approach to prevention and protection for individuals with ME/CFS, with a failure to recognise their specific vulnerabilities. This includes the increased potential for severe exacerbation of symptoms following vaccination, due to immune system dysregulation,3 as well as increased risk of post-viral complications. Emerging studies, including patient-led surveys, suggest people with ME/CFS have a higher risk of worsened ME/CFS if infected with COVID-19. For example, an ME Action survey of patients suggested: more than three quarters (76%) of respondents reported that COVID-19 made their ME/CFS symptoms worse. Over two-thirds of respondents said the worsening in symptoms had lasted more than 6 months.4
Adverse reactions – Despite being given adverse reaction data in November 2020, the Ministry of Health did not act to protect the vulnerable ME/CFS population from subsequent adverse reactions by allowing exemptions to further vaccination without penalty, and by continuing to advise and encourage clinicians to continue to advocate for continual vaccinations despite the harm benign caused at high frequency.
A belated lowered vaccine dose was offered after most individuals had taken the original dosage multiple times.
The process of reporting adverse effects (CARM) was overly complicated for ill people, and had to be processed through a GP, when GPs were over-run with COVID-19 cases and not seeing patients. Many did not officially report their adverse effects as a result.
Consequences of vaccine mandates in people with ME/CFS: A 2021 ANZMES survey of 395 people with an ME/CFS diagnosis highlights the impact of mandates, due to vaccine effect, on the state of ME/CFS illness/wellness, with 60% of respondents experiencing a level of deterioration in their health, with 3.1% experiencing a severe relapse, and a significant number experiencing reduced capacity to work and increased care requirements. People with ME/CFS also raised concerns over difficulties reporting adverse reactions due to the inability to get appointments with their GP and complex Centre for Adverse Reactions Monitoring (CARM) forms that were inaccessible due to neurological symptoms, such as brain fog, experienced by people with ME/CFS. It is also important to note that a small number of individuals with ME/CFS report an improvement in their chronic condition after vaccination, which experts propose is also related to the dysregulated immune system.
Lack of funding for long COVID support: Many people developed long COVID, however no extra funding was allocated for their care. The regional ME/CFS organisations were unable to access government funding to ensure that there was clinical, mental, and social wellbeing support for people developing long-term post-viral illness. Long COVID has put a strain on existing support services, due to a lack of suitable services available, forcing them to seek help from ME/CFS charities, such as ANZMES and regional support organisations [Complex Chronic Illness Support, ME/CFS Canterbury, ME Support NZ, MEISS Otago & Southland, and Rest Assured Charitable Trust]. Over 20% of Complex Chronic Illness Support referrals are for long COVID – with no dedicated funding to support this increase in demand for support services. People with long COVID and ME/CFS need increased recognition of the disabling nature of their conditions and increased support and this perspective is shared by international public health experts.5
Lack of consultation: ME/CFS organisations and experts were not invited to join the Expert Advisory Group for long COVID despite being the key source of support for people with long COVID due to decades of experience managing post-viral illness. ANZMES put forward names of expert clinicians and researchers and made considerable effort to make contact with decision-makers to no avail. At the time the public opinion was that this was a “new phenomenon” despite our organisations best efforts to advise otherwise. ANZMES was the first ME/CFS organisation in the world, founded in 1980. CCI Support was formed by ANZMES representatives the following year. ME/CFS Canterbury was formed in 1985. All these organisations have been dealing with diagnosis, treatment, and management of post-viral illness from the beginning.
Lack of clear communication about post-viral complications: Because of lack of consultation with experts in the field as mentioned above, there were no timely public health messages about the risk of developing long COVID or ME/CFS nor the need to rest to aid recovery and prevent complications. Brief belated guidance about resting was produced but missed the seriousness of what would happen if people ignored this guidance.
Health protections: Early health protections were beneficial to vulnerable individuals, these include; closing the borders to the Delta strain of the virus, isolation and travel restrictions, increased flexibility of services and workplaces (home delivery, work from home options), mask advice. However, removing the mask mandates and reducing infection isolation times were poor decisions that increased the spread of the virus. Global research shows that despite high vaccination rates reinfection continues to pose a significant threat of post-viral complications with implications for long-term socioeconomic burden.67
Protections have been removed but the pandemic is not over: The threat to public health, in NZ, is clearly ongoing with 5575 cases reported in the last week and 21 deaths attributed to the virus (as at 11/03/2024).8 78% more sick leave was taken in 2022 (than 2020) and wait times for emergency patients were exceeded by 95% of DHBs, in 2022.9 People with ME/CFS and long COVID are more vulnerable to the COVID virus, with hospitalisation a likely outcome, as well as a worsening of their existing symptoms and functional capacity. This has led to a greater number of people living with ME/CFS and long COVID in continued isolation, beyond original lockdowns, to protect themselves from an ongoing threat. This affects income, socialisation, mental health, and ability to carry out normal activities, such as grocery shopping or attending GP clinics. The removal of mask mandates acts as an additional barrier to healthcare access for vulnerable people with ME/CFS as there is an increased risk of infection with lack of certainty that staff will use high quality masks (N95/P2/FFP2) during consultations.
The Aotearoa COVID Action group has developed an 11 point COVID plan10 that includes practical steps to improve protection against the virus that would be of benefit to people with ME/CFS, such as mask mandates in high risk facilities, clean indoor air policies, increasing access to treatment and patient-led long COVID services. We support and encourage the implementation of these strategies.
Question 2: Moving forward – what lessons should we learn from your experiences so we can be as prepared as possible for a future pandemic?
Individuals with ME/CFS are often marginalised and their needs inadequately addressed in public health planning. Research highlights a disparity between government funding and level of disease burden for ME/CFS, in comparison to other chronic illnesses.11 There is a pressing need for comprehensive planning around post-viral illness for a future pandemic.
Post-viral illness is not new.
Research has shown that viral infections can trigger the onset of ME/CFS1213 and it is likely that the current pandemic will lead to an increase in cases in the years to come. Post-viral illness is not a new condition and we need to look at the past to plan for the future. Previous pandemics, such as the Spanish flu of 1918, the UK Royal Free Hospital viral outbreak of 1955, Incline village/Lake Tahoe, Nevada, USA mystery virus, and the Tapanui flu in New Zealand in 1984,14 have left a lasting legacy beyond the immediate impact of the viral outbreak. Studies and historical records indicate a pattern of post-viral illness among survivors.15
It is essential that public health authorities develop strategies for early identification, diagnosis, and management of post-viral illness, including appropriate support and resources for individuals with ME/CFS. International best practice guidelines recommend early diagnosis and intervention with a multidisciplinary team of healthcare professionals in order to improve outcomes.161718
If best practice guidelines are not followed appropriately there is great potential for harm because patients with post-viral illness who ignore or push through their symptoms can worsen their condition, often becoming bedridden.19
The World ME Alliance has issued a statement in response to the United Nations General Assembly, which adopted a Political Declaration on Pandemic Prevention, Preparedness and Response, calling for future pandemic planning to address infection-associated chronic conditions.20 Their statement highlights the urgency of the situation, according to recent research: “Globally, more than 65 million people are now living with long COVID, of whom 50% meet the criteria for a diagnosis of ME/CFS.”21
In New Zealand this is estimated conservatively to be around 400,000 people who will experience long COVID.22
Improving post-infectious disease management now will enable better preparedness for future outbreak events. This includes ensuring that information released by the health authority on ME/CFS and long COVID follow best practice. ANZMES recently sent best practice guidelines to Te Whatu Ora/Health NZ, the medical associations, councils, and schools and believe this document needs to be adopted immediately.
Funding for research and support services needs to be allocated by the government to address the demand occurring now. With these established practices and services in place and readily available in primary and secondary care, there will be no need to rush to set things up during the next outbreak, and new infections can be treated through the existing model. Appropriate tracking of prevalence and outcomes should be a routine part of this process.
We submit the following recommendations for consideration:
Inclusion of ME/CFS and long COVID as a priority population in public health planning and response efforts with tailored guidance and support for prevention and protection, with a focus on early intervention, education around the impact of ignoring best practice, and support for affected individuals.
Investment in research to better understand the relationship between viral infections, including COVID-19, and the onset of ME/CFS, as well as the development of effective treatments.
Investment in specific vaccine immune response research in people with ME/CFS and long COVID as a priority so that evidence-based advice can be provided. This would include using less reactogenic protein vaccines such as XBB Novavax over mRNA vaccines.
Make XBB Novavax or protein vaccines available for vulnerable populations such as ME/CFS and long COVID.
Ensure transparency around reported harms.
Increase access to funding and support for people with post-viral illness by reclassifying ME/CFS as a disability and removing eligibility barriers to financial aid.
ANZMES is utilised in an advisory capacity by all health and related agencies, and the best practice guidance is adopted by all.
Establishment of a post-viral or post-infectious centre of excellence, which includes:
Medical arm to assess and triage patients via telehealth.
Educational arm to provide the latest evidence-based information for health professionals, benefit assessors, insurers, employers, educational institutes.
Support arm to assist with financial, employers, educational adaptations.
Research arm to develop more effective management/treatment/cure that is prepared for immediate action, based on meaningful longitudinal studies – saving resources by avoiding unnecessary repetition of existing ME/CFS studies with long COVID cohorts.
ANZMES, as the National Advisory, already provides education, research funding and generation, and represents the national and global voice for people with ME (and supports those with long COVID and associated conditions) and is well positioned to take on the role of the Centre of Excellence with the appropriate infrastructure development through governmental funding and support.
By addressing the unique challenges and vulnerabilities faced by people with ME/CFS, we can ensure a more inclusive and effective public health response to future pandemics. We would welcome an opportunity to be involved in an advisory panel, to offer the wisdom and best practice requirements for this pandemic response and future viral outbreaks.
Who are ANZMES?
We are the National Advisory on ME in Aotearoa/New Zealand. With four decades of knowledge and experience, we are the trusted leaders in ME education, representation, and research. Our expertise comes from a reputable medical team of advisors, including a world renowned expert and MNZM recipient, a fellow of the Royal NZ College of General Practitioners (RNZCGP) and a network of academic researchers, clinicians, and representatives from the ME community. The executive committee comprises experts in their respective fields for governance, policy, leadership, representation, and education.
Always a trail-blazer, it was the first ME charity of its kind in the world, established in 1980, as ANZMES, to provide support, information dissemination, and representation, achieving past outcomes through dedication, passion, time, and knowledge of lived experience. Today, the organisation leads as a RNZCGP Continuing Medical Education (CME) Registered Provider, proud funder of vital research, and steward of the community voice.
We continue to disseminate evidence-based information nationally, and represent the ME voice globally as a founding member of the World ME Alliance through advocacy and leadership. ANZMES latest education programme – Know M.E. – is a video podcast and news series featuring up-to-date, evidence based research and information on ME and Post COVID Conditions.
References:
Davis, H.E., McCorkell, L., Vogel, J.M. et al. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 21, 133–146 (2023). https://doi.org/10.1038/s41579-022-00846-2 ↩︎
Hvidberg, et al (2015). The health related quality of life for patients with myalgic encephalomyelitis / chronic fatigue syndrome. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0132421 ↩︎
Walker, MOM, Peppercorn K, Kleffmann T, Edgar CD, Tate WP (2023) An understanding of the immune dysfunction in susceptible people who develop post viral fatigue syndromes Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Long COVID Medical Research Archives (accepted June 2nd). DOI:https://doi.org/10.18103/mra.v11i7.1.4083 ↩︎
ME Action. (2021). Report on the impact of Covid-19 on ME. https://www.meaction.net/2021/04/29/covid-19-has-worsened-our-me-report-survey-respondents/ ↩︎
Hereth B, Tubig P, Sorrels A, Muldoon A, Hills K, Evans N G et al. Long covid and disability: a brave new world BMJ 2022; 378 :e069868 doi:10.1136/bmj-2021-069868 ↩︎
Mulu Woldegiorgis, Gemma Cadby, Sera Ngeh, Rosemary Korda, Paul Armstrong, Jelena Maticevic, Paul Knight, Andrew Jardine, Lauren Bloomfield, Paul Effler. (2022).Long COVID in a highly vaccinated population infected during a SARS-CoV-2 Omicron wave – Australia. medRxiv 2023.08.06.23293706; doi: https://doi.org/10.1101/2023.08.06.23293706 ↩︎
K. Bach. (2022). New data shows long Covid is keeping as many as 4 million people out of work. https://www.brookings.edu/articles/new-data-shows-long-covid-is-keeping-as-many-as-4-million-people-out-of-work/ ↩︎
Health New Zealand/Te Whatu Ora. (2024). COVID-19 Current Cases. https://www.tewhatuora.govt.nz/our-health-system/data-and-statistics/covid-19-data/covid-19-current-cases/ ↩︎
Mirin, Arthur A., Dimmock, Mary E., and Jason, Leonard A. ‘Research Update: The Relation Between ME/CFS Disease Burden and Research Funding in the USA’. 1 Jan. 2020 : 277 – 282. ↩︎
Tate WP, Walker MOM, Peppercorn K, Blair ALH, Edgar CD. Towards a Better Understanding of the Complexities of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Long COVID. Int J Mol Sci. 2023 Mar 7;24(6):5124. doi: 10.3390/ijms24065124. PMID: 36982194; PMCID: PMC10048882. ↩︎
Cameron B., Flamand L., Juwana H., Middeldorp J., Naing Z., Rawlinson W., Ablashi D., Lloyd A. Serological and virological investigation of the role of the herpesviruses EBV, CMV and HHV-6 in post-infective fatigue syndrome. J. Med. Virol. 2010;82:1684–1688. doi: 10.1002/jmv.21873. ↩︎
George Dehner, Howard Phillips, In a Time of Plague: Memories of the ‘Spanish’ Flu Epidemic of 1918 in South Africa, Social History of Medicine, Volume 33, Issue 1, February 2020, Pages 343–344, https://doi.org/10.1093/shm/hkz093 ↩︎
National Institute for Health and Care Excellence(NICE). (2021). ‘Overview | Myalgic Encephalomyelitis (or Encephalopathy)/Chronic Fatigue Syndrome: Diagnosis and Management | Guidance | NICE’. NICE. https://www.nice.org.uk/guidance/ng206 ↩︎
Centers for Disease Control and Prevention. (2022). Information for Healthcare Providers. Understanding History of Case Definitions and Criteria. https://www.cdc.gov/me-cfs/healthcare-providers/case-definitions-criteria.html ↩︎
Mayo Clinical Proceedings (2021). Consensus Recommendations for ME/CFS: Essentials of Diagnosis and Management https://www.mayoclinicproceedings.org/article/S0025-6196(21)00513-9/fulltext ↩︎
Strassheim, Victoria; Newton, Julia L.; Collins, Tracy (February 5, 2021). “Experiences of Living with Severe Chronic Fatigue Syndrome/Myalgic Encephalomyelitis”. Healthcare. 9 (2): 168. doi:10.3390/healthcare9020168. ISSN 2227-9032. PMC 7914910. PMID 33562474. ↩︎
World ME Alliance. 32 organizations call for future pandemic preparedness to address infection-associated chronic conditions. 2023. https://worldmealliance.org/2023/10/31-organizations-call-for-future-pandemic-preparedness-to-address-infection-associated-chronic-conditions/ ↩︎
Davis, H.E., McCorkell, L., Vogel, J.M. et al. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 21, 133–146 (2023). https://doi.org/10.1038/s41579-022-00846-2 ↩︎
Russell L, Jeffreys M, Cumming J, Churchward M, Ashby W, Asiasiga L, Barnao E, Bell R, Cormack D, Crossan J, Evans H, Glossop D, Hickey H, Hutubessy R, Ingham T, Irurzun Lopez M, Jones B, Kamau L, Kokaua J, McDonald J, McFarland-Tautau M, McKenzie F, Noldan B, O’Loughlin C, Pahau I, Pledger M, Samu T, Smiler K, Tusani T, Uia T, Ulu J, Vaka S, Veukiso-Ulugia A, Wong C, Ellison Loschmann L (2022). Ngā Kawekawe o Mate Korona | Impacts of COVID-19 in Aotearoa. Wellington:Te Hikuwai Rangahau Hauora | Health Services Research Centre, Te Herenga Waka-Victoria University of Wellington. ↩︎
ANZMES President, Fiona Charlton spoke alongside Emeritus Professor Warren Tate from the University of Otago, and patient advocate Tom Harris to Kathryn Ryan on Nine to Noon on Radio New Zealand this morning.
The petition to reclassify Myalgic Encephalomyelitis to a disability is currently with the Health Select Committee, who are due to provide their recommendations to parliament in the coming months. This follows an oral submission to them by ANZMES on May 3rd 2023, a written submission presented in October 2022, and the petition with 6,444 signatures, submitted to parliament in September 2022.
ANZMES created this petition to draw attention to the fact that the system is not working for people with ME/CFS (pwME). Many fall through the cracks, many rely on whānau to care for them. Those who aren’t lucky enough to have family to care for them, experience post exertional malaise crashes regularly just trying to make a meal or do laundry. This means they’re in a constant state of unwellness with a myriad of over 100 symptoms. You can learn more about post exertional malaise on ANZMES World ME Day page.
Put simply:
ME/CFS fits the definition for disability BUT DOES NOT fit the criteria to access disability support services.
Those same support services are available under Long Term Support – Chronic Health Conditions BUT People with ME/CFS DO NOT fit the NASC* criteria to access them.
The system is not working for people with ME/CFS.
*NASC – Needs Assessment Service Coordination.
ME/CFS fits all definitions for disability created by the United Nations, The World Health Organisation, The Human Rights Act 1993, Statistics NZ, and the NZ government’s own definition (copied below). A disability is an impairment — physical, intellectual or sensory — that lasts for more than 6 months and limits your ability to carry out day-to-day activities.
pwME experience physical, cognitive, and sensory impairments. The condition for most, is chronic, for some it is lifelong. To be diagnosed with ME/CFS, one must experience at least a 50% reduction in ability to function (compared with pre-illness capacity).
ME/CFS fits the definition of disability. ME/CFS is a disability.
What would it mean to reclassify? A change in classification would be a lifeline to dedicated support and wider acknowledgement that this illness is disabling, providing fairer access to established support and care.
Being classified as a disability demonstrates the government understands how truly disabling this condition is. It legitimises ME/CFS as a physiological disease, which would foster the standardising of healthcare for pwME. Legitimising ME/CFS as the disability it is, should override and negate outdated opinions and treatments. It would provide pwME protection of rights as a disabled person.
It would ensure the government upholds its legal obligation to adhere to the United Nations (UNCRPD) Report (September 2022) which states that ME/CFS should be included in disability policies and supported by disability services.
It will enable pwME to fit into the criteria for NASC assessment for home help services. Access to services equates to intervention that promotes recovery or at the very least improvement in symptom management. When a person is constantly exerting beyond their energy capabilities, they crash. This is a health issue. NASC assessments are not conducted by the Ministry of Social Development, they are conducted through hospitals and the healthcare system. It is a healthcare issue.
ANZMES President, Fiona Charlton states “Members of Parliament are elected by the people, for the people. It is a democratic government’s role to ensure all policies, procedures, and programmes meet the needs of all New Zealanders. People with ME/CFS are New Zealanders. Yet, their needs are not being met. There is no-one in parliament representing us. We have to advocate for ourselves, yet who is listening? Who in parliament will stand up for and advocate for the needs of pwME? Who will ensure our needs are met?”
In 2012, following a petition by ANZMES Executive Committee member, Wendy Matthews, the then Health Select Committee made the recommendation to reclassify ME/CFS as a disability.
This was NOT implemented by government.
Fiona Charlton states “We have hope that the Health Select Committee will once again make the recommendation to reclassify ME/CFS as a disability. However this time, we also urge these committee members to use their roles within parliament to ensure the government implements the advice.”
ANZMES invite members of parliament to speak with them. ANZMES has the knowledge, expertise, and lived experience. ANZMES has world-renowned clinicians on the executive committee and medical team, and researchers like Emeritus Professor Warren Tate are available for discussions.
ANZMES current Royal NZ College of General Practitioners (RNZCGP) CME (continuing medical education) accredited series: Know M.E. is freely available to all health professionals seeking to understand the biomedical, physiological nature of ME/CFS and evidence-based management strategies.
The information is available for a considered, evidence-based response from parliament to meet the needs of people with ME/CFS. ANZMES offers solutions in its written submission (October 2022), and written report submitted to Health and Disability Ministers and Commissioners in July 2022. You can view the oral submission here: anzmes-speaks-to-parliament.
ANZMES looks forward to the recommendations from the Health Select Committee in the coming months.
ANZMES is dedicated to continually advocating, supporting, educating, and funding research for pwME.
Who are ANZMES? The Associated New Zealand Society for ME/CFS (ANZMES) have been providing information, awareness for ME/CFS, funding research, and advocating for people with ME/CFS for the past 43 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership. ANZMES is a RNZCGP registered provider for continuing education. Health professionals can earn CME/CPD credits with ANZMES latest education programme – Know M.E. – a video podcast and news series featuring up-to-date, evidence based research and information on ME/CFS and Post COVID Conditions.
The Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) supports the new position paper on the Lightning Process by the World ME Alliance and does not endorse the Lightning Process for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).
The Lightning Process is a programme loosely based on concepts of neuro linguistic programming (NLP) and cognitive behaviour therapy (CBT) that is set up commercially and currently marketed as a cure for ME/CFS. This claim is not backed by scientific evidence and ANZMES shares the view of the World ME Alliance that the promotion of this programme is likely to do harm.
The National Institute for Health and Care Excellence (NICE), in the UK, revised their guidelines for the diagnosis, treatment, and management of ME/CFS stating that the lightning process should not be used as a treatment and they no longer recommend CBT. These changes reflect a shift from an outdated perspective that ME/CFS was a psychological condition and follows evidence from over 200 studies showing poor efficacy for this treatment approach.
ANZMES President, Fiona Charlton says, “there is a growing body of evidence that shows that ME is driven by physiological changes not psychological ones and telling people that they can talk themselves out of this condition, within three days, could be very harmful.
“We know that if people with ME ignore their symptoms and push themselves this can make things worse, sometimes to the point of needing hospital care.”
ANZMES agrees with the World ME Alliance who highlight in their statement that people with ME/CFS are vulnerable to exploitation due to a lack of effective treatment where programmes like the Lightning Process are just filling this void.
People living with Long COVID are also being drawn into this treatment as this is now an extension of their claims to cure ME/CFS.
Other concerns with the Lightning Process include a bias in efficacy studies, including conflicts of interest, a reported secrecy where participants are told not to speak about the programme or their symptoms and a level of shame and guilt for those who do not recover within the three days of treatment.
Charlton says, “we want to ensure that if we are endorsing a treatment for ME that robust evidence supports efficacy and this is just not the case with LP.
“What we do know is that a treatment approach that is focussed around symptom management is shown to help with the relapsing nature of ME.”
ANZMES acknowledges that neurological symptoms, such as depression and anxiety can be a part of ME/CFS and may benefit from supportive therapies but people have the right to unbiased, impartial information when being offered these treatments.
***********************
The Lightning Process was developed and trademarked by British osteopath and hypnotherapist Phil Parker.
ANZMES has been providing information, building awareness, funding research, and advocating for people with ME/CFS for the past 42 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice, globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership.
At the request of the ME/CFS community, ANZMES has issued a survey relating to reactions experienced by the community to the COVID-19 Pfizer BioNTech vaccine. ANZMES also sought to ascertain prevalence of Long COVID and COVID-19 infection in the community. The opportunity was also utilised for respondents to express interest in participating in a potential fractionated dosing trial.
This report contains preliminary findings for responses received from 21st October 2021 to 10th November 2021. This survey is still open to capture experiences after these dates, as vaccination decisions are ongoing.
Please note that this survey is classed as a self-report questionnaire which seeks to ascertain the subjective experience of people with ME/CFS and co-morbid conditions. The information collected is therefore anecdotal data. No clinical research has been conducted.
Respondents
395 respondents identify with an ME/CFS diagnosis
144 with Fibromyalgia (some overlap with ME/CFS)
19 with COVID-19
5 diagnosed with, and 32 suspect, Long COVID
The majority of respondents have a clinical diagnosis of ME, with 25 self-diagnosed. Most are unsure as to which diagnostic criteria for ME was used.
Some questions have less respondents, therefore numbers are indicated in the relevant sections.
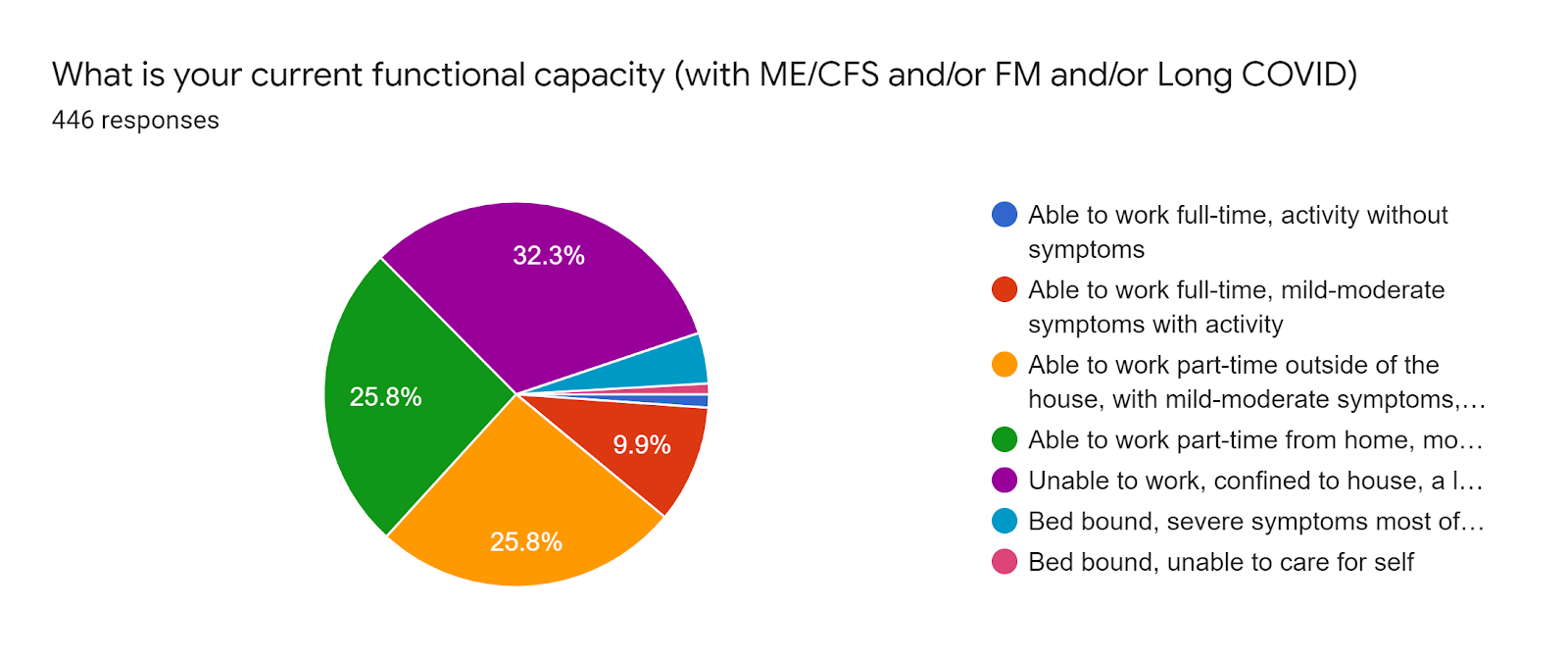
Functional capacity (pre-vaccination)
32.3% (144 individuals) are unable to work, confined to their home with a lot of rest required.
25.8% (115) are able to work part-time at home.
25.5* (115) are able to work part-time outside of the house.
9.9% (44) are able to work full-time with mild-moderate symptoms with activity. 1.1% (5) are able to work full-time without symptoms. * These respondents were mostly COVID-19 infection or Long COVID respondents without ME/CFS.
4.3% (19) are bedbound most of the time.
0.9% (4) are bedbound and unable to care for themselves.
Vaccination rates
The majority of respondents have had two doses of the Pfizer vaccination.
64.5% (296) two doses.
16.1& (74) single dose.
19.2% (88) have not been vaccinated.
Of the 296 with two doses, the duration between doses was 6 weeks or more for 166 individuals and 3 weeks for 130.
Pattern for capacity and reaction
These findings suggest that the more disabling the ME/CFS symptoms, the more prone to a relapse after vaccination but that relapse can occur at any functional capacity state for pwME. This was analysed when there were 241 responses.
Temporarily worsened
Improved
No change
Worsened into relapse
Worsened beyond illness
Not vaccinated
No answer
Part-time work home
22
8
7
9
1
14
2
Part-time outside house
22
3
17
14
0
12
2
Full-time work mild-mod with activity ME FM Long COVID/COVID
3 2 0
0 0 2
4 1 3
3 1 0
0 0 0
2 0 1
2 0 5
Unable to work, confined to house
23
6 3 temp
15
18
7
8
7
Bedbound mostly
2
0
0
3
0
1
1
Bedbound unable to care for self
0
0
0
1
0
1
1
Overall ME
72
20
43
48
8
30
20
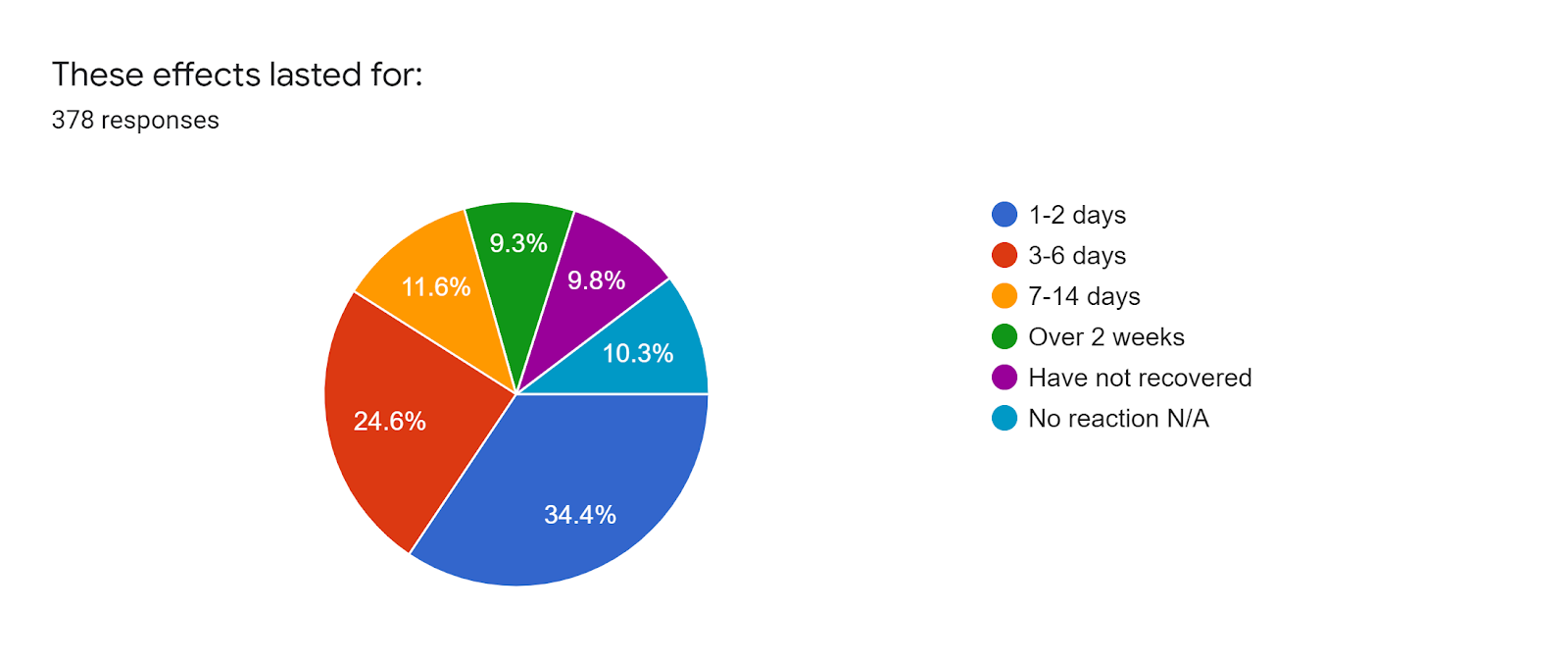
First dose vaccination reaction and duration
There were 39 individuals who did not experience any symptoms. For those who did experience reactions to the first dose of the vaccine, these were consistent with the expected normal immune response, e.g.:
sore at injection site (300)
tired/fatigued (219)
Headache (142)
nausea/gastrointestinal issues (62)
fever/chills (56)
Swollen lymph nodes (46)
Sleep issues/insomnia (44)
5 people experienced heart palpitations and/or anxiety 3 people experienced skin sensitivity and/or allergy flares, with 2 people experiencing brain fog/cognitive issues.
For most people (130) these symptoms lasted 1-2 days.
For 93 individuals it lasted 3-6 days.
44 experienced symptoms for 7-14 days.
35 for over 2 weeks.
37 have not recovered.
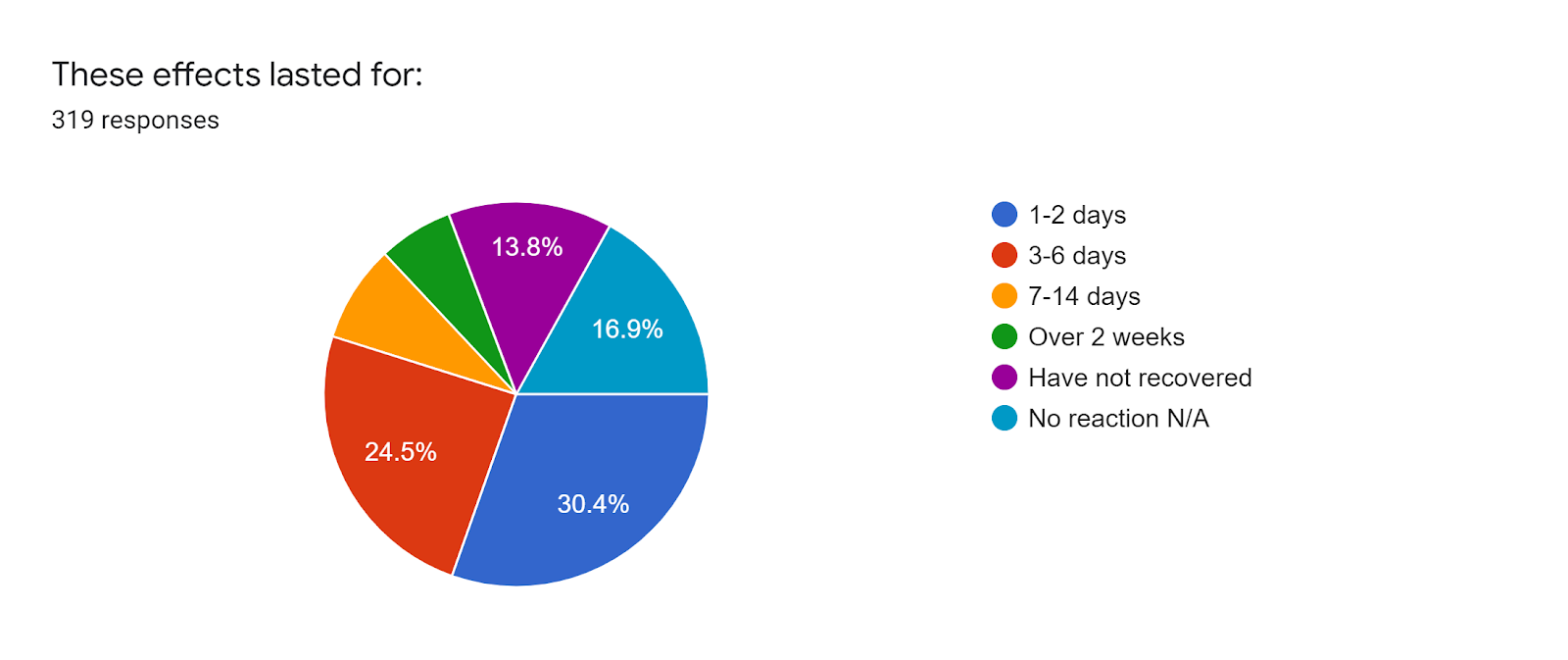
Second dose reaction and duration
As has been reported by the general public, the findings from this survey suggest that pwME also experienced more adverse reactions to the second dose of the Pfizer vaccine. However there were 54 individuals who did not experience any symptoms.
For 97 individuals these symptoms lasted 1-2 days.
For 78 individuals it lasted 3-6 days.
26 experienced symptoms for 7-14 days.
20 for over 2 weeks.
44 have not recovered.
Vaccine effect on state of illness/wellness for 359 respondents
137 (38.1%) experienced no change/stay the same
118 (32.9%) temporarily worsened but have returned to baseline
71 (19.8%) worsened and not returned to baseline – relapsed
22 (6.1%) improved
11 (3.1%) worsened beyond anything experienced in illness to date – severe relapse
289 respondents did not have any new symptoms that they could attribute to the vaccine.
52 stated that they had new symptoms that they could attribute to the vaccine. These symptoms tended to be over-activation of the immune response, e.g. sore throat, swollen neck glands, allergy reactions. Of these 52 – 4 individuals have gastrointestinal issues, 2 experienced more fatigue whilst 1 indicated improved energy.
Clinical care
From 383 responses 314 (82%) were not offered clinical care during vaccination, 15 (3.9%) were offered clinical care, 19 (5%) were unsure. 25 people asked for specific clinical care during the vaccination process. Of those offered clinical care the options were 30 minute observation rather than the normal 15, separate areas with direct nurse observation. Others were advised by their GPs to rest and take antihistamines pre- and post-vaccination.
Caregiving requirements
From 353 respondents 50 require ongoing caregiving for their ME/CFS and/or FM and 70 required care after vaccination. 244 people do not require caregiving before and 230 after.
Fractionated dosing interest
If fractionated / lower dosing had been an option, of 115 responses 48 stated they would have considered it, 23 said they would not consider it and 44 were unsure.
Of 88 responses for those reluctant to have the vaccine, 57 would consider lower dosing options, 10 would not, and 21 were unsure.
Of 124 responses to indicate interest in participation in a potential trial into fractionated dosing, 61 responded that they are interested, 31 may be interested, and 32 are not.
Antihistamine usage
Of 115 responses 45 did not take any pre- or post-vaccination, 70 did.
Reasons for not being vaccinated
Of 1Anxiety/worry/fear about potential adverse reactions, previous adverse reactions to other vaccines, concern about the safety of the vaccine, high ME/CFS symptomatology, chemical sensitivities/MCS/MCAS, not currently well enough to risk adverse reactions.
COVID-19 / Long COVID
19 respondents have been diagnosed with SARS-CoV-2 (COVID-19) infection.
169 respondents have had COVID-19 tests.
5 people have been diagnosed by a medical professional with Long COVID.
32 people suspected they have Long COVID after a viral infection due to ongoing or lingering classic COVID-19 symptoms and having been connected to a location of interest, an overseas hot zone of infection, or have remained unwell after experiencing a viral infection that has not been confirmed as COVID but has the same symptoms.
May 12th is the Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) International Awareness Day.As we mark this day each year, we highlight how you can support the millions of people globally (and at least 25,000 here in NZ) who suffer from ME/CFS. We mark this day on Florence Nightingale’s birthday, because it is thought that she developed ME/CFS after an infection contracted during the Crimean War.
ME/CFS is a serious, disabling, long-term disease which affects multiple bodily systems (immune, endocrine, neurological and autonomic). [1] The World Health Organisation classified ME/CFS as a neurological disease back in 1969. Despite this, ME/CFS has often been misunderstood, stigmatised as psychosomatic, and underfunded. Today we have a much clearer understanding of the biological basis for the disease through research from the likes of Harvard, Stanford, Cornell, and DePaul universities in the USA, and our very own Emeritus Professor Warren Tate of the University of Otago.
This year, with COVID-19 still present globally, we also want to direct attention to the estimated 25-35% of cases [2] who have not recovered from the virus. Those people who are still unwell 12 weeks after the expected recovery period, are classed as having “Long COVID” and some go on to receive a diagnosis of ME/CFS as well.
There are similarities between ME/CFS and Long COVID (some symptoms overlap):
ME-CFS *
Long COVID *
Severe fatigue with post-exertional malaise
Fatigue
Cognitive dysfunction (brain fog, memory lapses)
Brain fog
Gastrointestinal issues
Gastrointestinal issues
shortness of breath
shortness of breath
Fevers/Chills
Fevers/Chills
* this is not an exhaustive list of symptoms
This is not surprising because a large percentage of those with ME/CFS, develop it after not recovering from a virus such as Epstein Barr/Mononucleosis, SARS-CoV, etc., or from other infectious illnesses such as Lyme disease (Mayo Clinic, 2020).
What does it mean to have ME/CFS? The list above is not exhaustive. Those with ME/CFS also experience significant deep muscular pain and can also experience a varying degree of symptoms that link to dysfunction of distinct systems in the body [3]:
ME/CFS is a chronic illness, meaning it is long term.
It can be classed as having three distinct levels of symptom severity [4]:
Mild – at least a 50% decrease in pre-illness activity but may still be able to achieve part-time work and activities
Moderate – mostly housebound (can’t attend work/school or do normal activities)
Severe – bedbound and dependent on help with all daily care (this occurs in approximately 25% of all ME/CFS cases).
ME/CFS knows no bounds – it affects all ages, ethnicities, genders and socioeconomic groups. At this point in time there is no cure, but there is research going on to develop a suitable treatment based on previous research into root cellular causes and dysfunction. Currently Prof. Tate is working on comparing the molecular similarities between ME/CFS and Long COVID patients recruited through the practice of collaborating physician Dr. Rosamund Vallings, in order to not only understand the underlying pathophysiology (root causes and malfunctions) but also to discover potential treatments. [5] Dr. Tate states “Unlike ME/CFS patients who have had their illness from six months to over 40 years in some cases, the long COVID group with post-viral fatigue have been unwell for a relatively short time (up to a year). This is early in the course of what could be a lifelong disease like ME/CFS, so now is the best time to research therapeutic options that might alleviate – and even reverse – the disease.”
How can you help? 5 ways:
1 Educate – This awareness day, please take time to learn more about ME/CFS and Long COVID by visiting links suggested in this article, by perusing the rest of the ANZMES website and joining our Facebook page: If you or someone you know has ME/CFS share your personal stories with others, on social media, and take time to listen to others’ stories.
2 Support – on May 12th wear BLUE to raise awareness and show support for people with ME/CFS, their families and caregivers as well as the researchers who study ME/CFS. Please use social media to spread information about ME/CFS – share this article, and post photos of you and your family and friends wearing blue. Use hashtags #ISTANDforMECFS #MECFSUnity #ANZMES #BLUEforMECFS #millionsmissing #thelonghaulandME #MEandCOVID #solveMECFS
3 Share our posters and memes and this blog on social media, with friends and family, with your local GP and healthcare providers, and lets show all those living with ME/CFS and Long COVID that they are not alone, they are heard and supported.
Posters:
4 Lobby your local MP to demand that:
Evidence-based health guidelines are used by all government agencies to ensure accurate information about ME/CFS for timely diagnosis and management and access to necessary services (including home help and supported living payments)
Dedicated research funding is set aside for treatment development
ME/CFS is reclassified as a disability so that those unable to work due to the severity of their illness are able to gain access to the services they need.
5 Join our organisation to receive lobbying letter templates, information sheets, and access to the latest news and developments.
We look forward to seeing your presence on social media this May 12th for ME/CFS International Awareness Day 2021. Thank you.
May 12 marks the international Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Awareness Day, on Florence Nightingale’s birthday (as it is thought she developed ME/CFS after an infection contracted during the Crimean war). Each year on this day ANZMES (the Associated New Zealand ME Society) seeks to provide education and build awareness, as well as advocate for and support those with ME/CFS and their families. This year, with COVID-19 still present globally, attention must also be on those diagnosed with Long COVID. Long COVID will present new challenges. Many of those challenges have already been faced by the ME/CFS community.
Myalgic Encephalomyelitis (ME/CFS) is a serious long-term illness causing disabling symptoms exacerbated by both mental and physical exertion [1]. Despite the person often appearing ‘well’ there are debilitating symptoms that include but are not limited to: incapacitating exhaustion, post-exertional malaise, pain, sleep disturbances, cognitive and gastro-intestinal issues, and orthostatic intolerance (severe light-headedness when standing). The illness affects all genders, races and ethnicities. It affects children, those at university still studying, those just entering the workforce, mums and dads juggling home and work and people at the peak of their careers, right up to the elderly who already have other struggles. Some will recover after some months or years, but those who are still sick two years after onset are likely to suffer this illness for the rest of their lives.
In NZ there are at least 25,000 people living with ME/CFS – that’s approximately 1 in every 250 adults and 1 in every 134 youth. It commonly has acute onset (occurs suddenly) after a viral illness (e.g. Epstein Barr/Mononucleosis and SARS-CoV) [2]. The COVID-19 virus (SARS-CoV-2) has resulted in a post-viral syndrome for an estimated 25-35% of all cases [3]; a syndrome similar in symptomatology to ME/CFS. Those still unwell twelve weeks after onset [4], are classed as having Long COVID and some go on to receive an ME/CFS diagnosis too. This means the prevalence of ME/CFS in NZ and worldwide is increasing.
There is currently no cure for ME/CFS. However researchers around the world, including Cornell, Stanford and Harvard Universities in the USA, are working to understand the disease, find a diagnostic test and develop more treatments. Despite this, research is woefully underfunded. In the last year The European Union has called for more funding [7]. Researchers here in New Zealand, including a team led by the Rutherford Medal winner Emeritus Professor Warren Tate of the University of Otago, have to rely on donations from people with ME/CFS, their families and organisations such as ANZMES. One such study also funded by Brain Research NZ is to assess the pathophysiological similarities between ME/CFS and those diagnosed with Long COVID [8]. Dr. Tate states “Unlike ME/CFS patients who have had their illness from six months to over 40 years in some cases, the long COVID group with post-viral fatigue have been unwell for a relatively short time (up to a year). This is early in the course of what could be a lifelong disease like ME/CFS, so now is the best time to research therapeutic options that might alleviate – and even reverse – the disease.” [9]
The increase of people with ME/CFS and Long COVID has far-reaching repercussions. For society this means a loss of available people in the workforce and further burdens to the public health system. For the individual it means increased medical costs and a loss of salary. Between 40-81% of those with ME/CFS are unable to maintain employment due to fluctuating, disabling symptoms [10]. A decrease in social contact can result in social isolation, loneliness, and diminished quality-of-life [11]. Even those with ‘mild’ symptoms experience at least a 50% decrease in pre-illness activity [12]. Imagine being unable to meet your friend for coffee at the local café because you don’t even have the energy to shower and dress. Or consider being housebound, not just for a few weeks (like many kiwis experienced during lockdown) but for decades or a lifetime. Imagine the teenager who cannot physically attend school and has to complete coursework from bed. Or picture not being able to play with your children or grandchildren, and missing out on seeing them in school plays and sports. This is the reality for many with ME/CFS.
This year, on the International ME Awareness Day (May 12th), please think about those with ME/CFS and Long COVID, who face ongoing isolation and difficulties associated with living with a chronic illness.
Resources are available for patients, carers, teachers and health professionals through the Associated New Zealand ME Society (ANZMES) at www.anzmes.org.nz.