ANZMES President, Fiona Charlton spoke alongside Emeritus Professor Warren Tate from the University of Otago, and patient advocate Tom Harris to Kathryn Ryan on Nine to Noon on Radio New Zealand this morning.
You can view the Radio New Zealand interview news bulletin here: https://www.rnz.co.nz/national/programmes/ninetonoon/audio/2018892129/the-fight-to-get-me-chronic-fatigue-syndrome-classified
You can listen to the interview episode here:
https://www.rnz.co.nz/audio/player?audio_id=2018892129
The petition to reclassify Myalgic Encephalomyelitis to a disability is currently with the Health Select Committee, who are due to provide their recommendations to parliament in the coming months. This follows an oral submission to them by ANZMES on May 3rd 2023, a written submission presented in October 2022, and the petition with 6,444 signatures, submitted to parliament in September 2022.
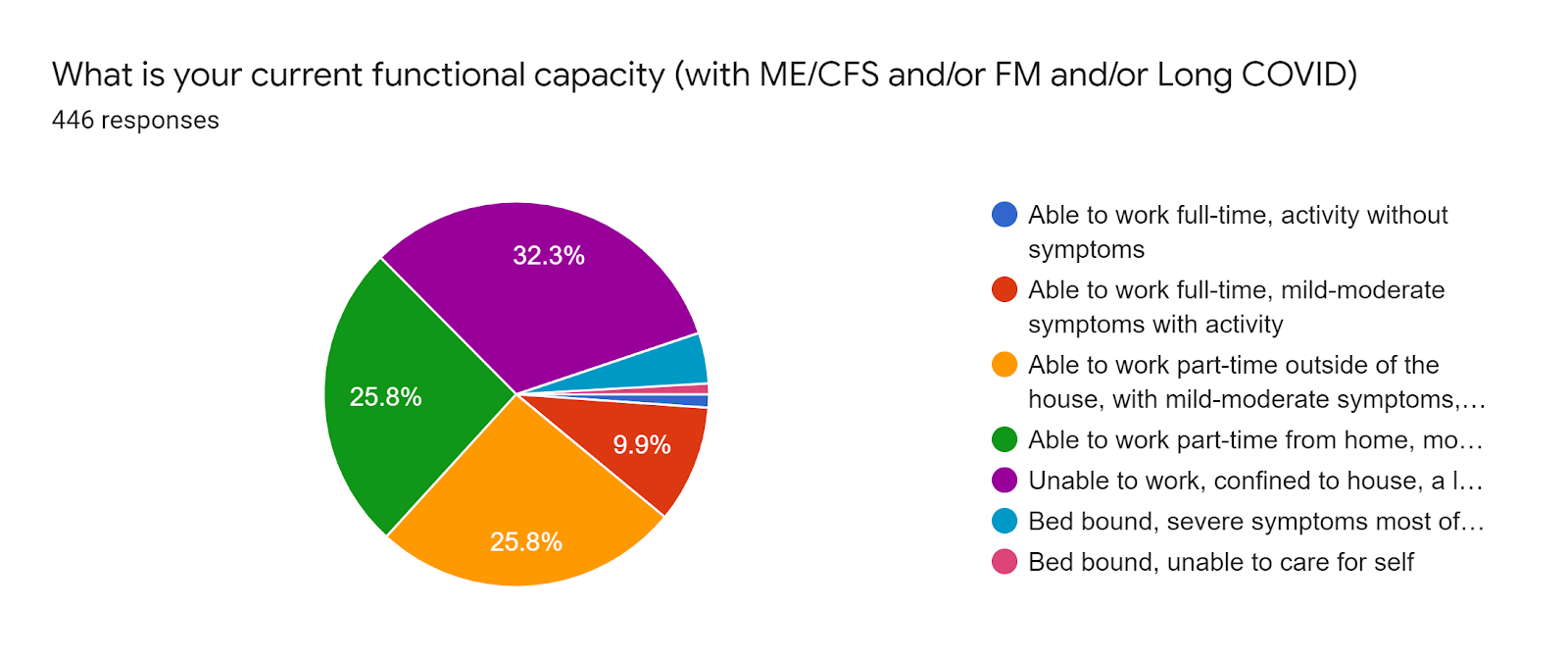
ANZMES created this petition to draw attention to the fact that the system is not working for people with ME/CFS (pwME). Many fall through the cracks, many rely on whānau to care for them. Those who aren’t lucky enough to have family to care for them, experience post exertional malaise crashes regularly just trying to make a meal or do laundry. This means they’re in a constant state of unwellness with a myriad of over 100 symptoms. You can learn more about post exertional malaise on ANZMES World ME Day page.
Put simply:
ME/CFS fits the definition for disability
BUT
DOES NOT fit the criteria to access disability support services.
Those same support services are available under Long Term Support – Chronic Health Conditions
BUT
People with ME/CFS DO NOT fit the NASC* criteria to access them.
The system is not working for people with ME/CFS.
*NASC – Needs Assessment Service Coordination.
ME/CFS fits all definitions for disability created by the United Nations, The World Health Organisation, The Human Rights Act 1993, Statistics NZ, and the NZ government’s own definition (copied below).
A disability is an impairment — physical, intellectual or sensory — that lasts
for more than 6 months and limits your ability to carry out day-to-day activities.
pwME experience physical, cognitive, and sensory impairments.
The condition for most, is chronic, for some it is lifelong.
To be diagnosed with ME/CFS, one must experience at least a 50% reduction in ability to function (compared with pre-illness capacity).
ME/CFS fits the definition of disability. ME/CFS is a disability.
What would it mean to reclassify?
A change in classification would be a lifeline to dedicated support and wider acknowledgement that this illness is disabling, providing fairer access to established support and care.
Being classified as a disability demonstrates the government understands how truly disabling this condition is.
It legitimises ME/CFS as a physiological disease, which would foster the standardising of healthcare for pwME. Legitimising ME/CFS as the disability it is, should override and negate outdated opinions and treatments. It would provide pwME protection of rights as a disabled person.
It would ensure the government upholds its legal obligation to adhere to the United Nations (UNCRPD) Report (September 2022) which states that ME/CFS should be included in disability policies and supported by disability services.
It will enable pwME to fit into the criteria for NASC assessment for home help services. Access to services equates to intervention that promotes recovery or at the very least improvement in symptom management. When a person is constantly exerting beyond their energy capabilities, they crash. This is a health issue. NASC assessments are not conducted by the Ministry of Social Development, they are conducted through hospitals and the healthcare system. It is a healthcare issue.
ANZMES President, Fiona Charlton states “Members of Parliament are elected by the people, for the people. It is a democratic government’s role to ensure all policies, procedures, and programmes meet the needs of all New Zealanders. People with ME/CFS are New Zealanders. Yet, their needs are not being met. There is no-one in parliament representing us. We have to advocate for ourselves, yet who is listening? Who in parliament will stand up for and advocate for the needs of pwME? Who will ensure our needs are met?”
In 2012, following a petition by ANZMES Executive Committee member, Wendy Matthews, the then Health Select Committee made the recommendation to reclassify ME/CFS as a disability.
This was NOT implemented by government.
Fiona Charlton states “We have hope that the Health Select Committee will once again make the recommendation to reclassify ME/CFS as a disability.
However this time, we also urge these committee members to use their roles within parliament to ensure the government implements the advice.”
ANZMES invite members of parliament to speak with them. ANZMES has the knowledge, expertise, and lived experience. ANZMES has world-renowned clinicians on the executive committee and medical team, and researchers like Emeritus Professor Warren Tate are available for discussions.
ANZMES current Royal NZ College of General Practitioners (RNZCGP) CME (continuing medical education) accredited series: Know M.E. is freely available to all health professionals seeking to understand the biomedical, physiological nature of ME/CFS and evidence-based management strategies.
The information is available for a considered, evidence-based response from parliament to meet the needs of people with ME/CFS. ANZMES offers solutions in its written submission (October 2022), and written report submitted to Health and Disability Ministers and Commissioners in July 2022. You can view the oral submission here: anzmes-speaks-to-parliament.
ANZMES looks forward to the recommendations from the Health Select Committee in the coming months.
ANZMES is dedicated to continually advocating, supporting, educating, and funding research for pwME.
Who are ANZMES?
The Associated New Zealand Society for ME/CFS (ANZMES) have been providing information, awareness for ME/CFS, funding research, and advocating for people with ME/CFS for the past 43 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership. ANZMES is a RNZCGP registered provider for continuing education. Health professionals can earn CME/CPD credits with ANZMES latest education programme – Know M.E. – a video podcast and news series featuring up-to-date, evidence based research and information on ME/CFS and Post COVID Conditions.