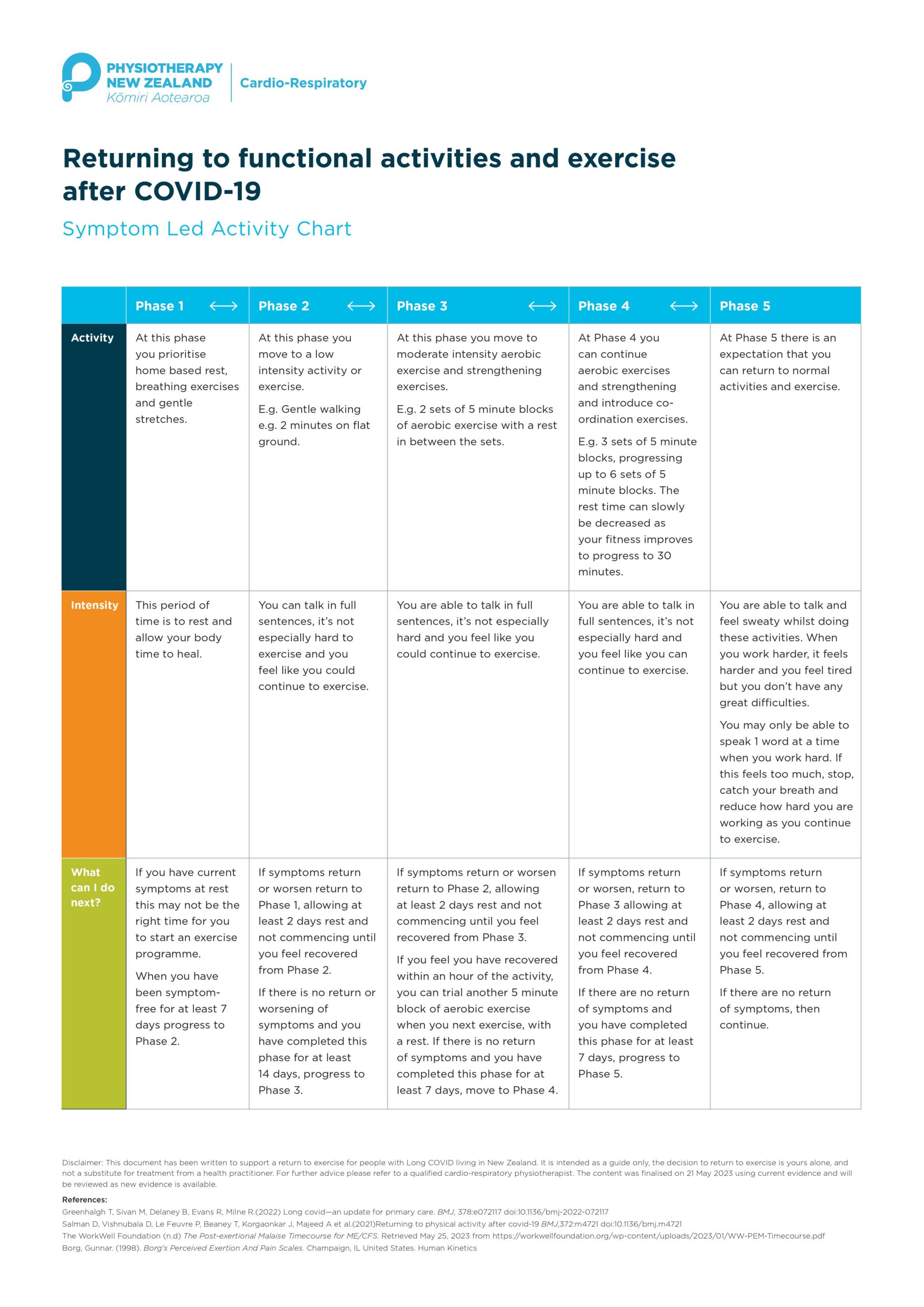
Physiotherapy New Zealand has provided ANZMES with a flow chart for the return to exercise advice in the Long COVID space.
Please find attached the flow chart designed for health care professionals to be supported in giving safe exercise advice.


Physiotherapy New Zealand has provided ANZMES with a flow chart for the return to exercise advice in the Long COVID space.
Please find attached the flow chart designed for health care professionals to be supported in giving safe exercise advice.
For immediate release – 18/09/2023
Two New Zealand researchers have been chosen to receive the Associated New Zealand Myalgic
Encephalomyelitis Society (ANZMES) annual grant of $25,000 to undertake vital research into
increasing understanding of Myalgic Encephalomyelitis (ME, also known as Chronic Fatigue
Syndrome), in Aotearoa.
ANZMES, the National Advisory on ME, launched the new grant and scholarship programme for
postgraduate students and academic researchers this year – aimed at supporting those
interested in researching ME and long COVID. With six funding opportunities available, ANZMES
encouraged applications from those seeking to undertake research that furthers understanding,
treatment, or prevention of ME and long COVID, including two $25,000 grants and four $5,000
scholarships to support research and study costs.
The 2023 Grant recipients are:
● Principal investigator: Dr. Nicholas Bowden, Research Fellow, Department of Women’s and
Children’s Health, University of Otago (pictured below. Photo credit: University of Otago).

Co investigators: Keith McLeod, Associate Principal, Kōtātā Insight.
Dr. Rosamund Vallings, retired GP, Howick Health and Medical
Centre.
Emeritus Professor Warren Tate, Department of Biochemistry,
University of Otago.
Professor Barry Taylor, Department of Women’s and Children’s
Health, University of Otago.
Francisca Anns, PhD Candidate, COMPASS Research Centre,
University of Auckland.
The study will investigate the health, labour market, and social service use of people with
ME, in NZ, through a population study.
Dr. Bowden says, “we are excited and grateful to receive this grant to undertake what we believe
is an important piece of research, providing foundational population-level evidence on health,
labour market, and social service outcomes for those with ME/CFS in Aotearoa/New Zealand for
the first time.”
● Principal investigator: Dr. Lynette Hodges, Senior Lecturer School of Sport, Exercise and
Nutrition, Massey University, Registered Clinical Exercise Physiologist (pictured below.
Photo credit: Massey University).

The study will investigate activity and energy management and
the hallmark symptom post-exertional malaise (PEM), in people
with ME through an observational study that assesses exertion
during normal daily activities of living, such as doing dishes or
laundry.
Dr. Hodges says, “I am so thrilled to learn that my research
application was chosen. I hope that this research will be able
to be of benefit to those with ME/CFS. As a Clinical Exercise
Physiologist, I am keen to help people live their best lives and hope that this study will develop a
better understanding of how activities of daily living affect the physiology of those living with
ME/CFS.”
Dr. Bowden and Dr. Hodges will both receive the $25,000 Grants through their respective
universities, to carry out their research projects.
ANZMES President, Fiona Charlton, says, these investments will help facilitate a crucial source of
New Zealand based research, furthering our understanding of the disabling condition.
“We are really pleased by the calibre of the work proposed by both recipients.
“With Dr. Bowden’s work, for the first time we will have a foundational study that offers insight into the lives and experiences of people with ME in Aotearoa.
“We understand the burden of disease from an international research perspective but New
Zealand based studies are lacking.
“Research into PEM and activity management will also be invaluable for both patients and health
professionals and will have implications for long COVID management and recovery.
“While we did not receive any scholarship applications, we encourage postgraduate students to
consider their Masters/PhD topics now, for next year’s funding round. In programs with relatively
low costs, scholarships can be used to help pay fees or study and living expenses,” says Charlton.
ME is a complex, debilitating and often misunderstood medical condition and although millions of
people suffer with the illness worldwide, including a significant population in New Zealand, there
is remarkably little research or funding available.
This ANZMES funding programme was made possible by the generous support of members.
The Grant was awarded by ANZMES on the recommendation of their Grants and Scholarships
Subcommittee.
Next year’s funding applications open May 31st.
Visit anzmes.org.nz for more information, grant regulations, and application forms.
What is ME/CFS?
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is often triggered by a viral
illness and involves overwhelming fatigue and other symptoms that range in severity as it affects
many body systems, such as the immune, neuroendocrine and autonomic nervous system.
The key characteristic of ME/CFS is post exertional malaise (PEM) which presents 12-48 hours
after exertion, and can result in days to weeks of exacerbated symptoms. For the very severe, this
exertion can be simply trying to speak, or eat.
Who are we?
We are the National Advisory on ME in Aotearoa/New Zealand. With four decades of knowledge
and experience, we are the trusted leaders in ME education, representation, and research. Our
expertise comes from a reputable medical team of advisors, including a world renowned expert
and MNZM recipient, a fellow of the Royal NZ College of General Practitioners (RNZCGP) and a
network of academic researchers, clinicians, and representatives from the ME community. The
executive committee comprises experts in their respective fields for governance, policy,
leadership, representation, and education.
Always a trail-blazer, it was the first ME charity of its kind in the world, established in 1980, as
ANZMES, to provide support, information dissemination, and representation, achieving past
outcomes through dedication, passion, time, and knowledge of lived experience. Today, the
organisation leads as a Royal New Zealand College of General Practitioners (RNZCGP) Continuing
Medical Education (CME) Registered Provider, proud funder of vital research, and steward of the
community voice.
We continue to disseminate evidence-based information nationally, and represent the ME voice
globally as a founding member of the World ME Alliance through advocacy and leadership.
ANZMES latest education programme for health professionals – Know M.E. – is a video podcast
and news series featuring up-to-date, evidence based research and information on ME and Post
COVID Conditions.
For immediate release – 22/08/2023

Petition response: ANZMES welcomes Committee recommendations for improved access to disability services for people with ME/CFS
ANZMES, the National Advisory on Myalgic Encephalomyelitis (ME), has welcomed the Health Select Committee’s (HSC) response to its petition delivered in September 2022, calling on the Government to reclassify ME as a disability.
The Health Select Committee presented its report to parliament on 17th August 2023, sending a strong message acknowledging ANZMES petition to reclassify ME – also known as Chronic Fatigue Syndrome (CFS) – as a disability with the recommendation that eligibility criteria for disability services be amended.
The 10 page HSC Report recommends that the Government take note stating “we understand that ME/CFS meets the Government’s definition of a disability. We therefore, encourage Whaikaha to consider amending its eligibility criteria to enable people with ME/CFS to access Whaikaha-funded disability support services.”
The Report also acknowledged concerns raised by ANZMES that the current classification and system is flawed with complicated assessment processes and policies and disparity between regions causing access inequality.
ANZMES President Fiona Charlton says the acknowledgement and recommendations are “a step in the right direction.”
“The struggle is real for so many people with ME and improving access to Whaikaha-funded support services could give so much relief to them.”
The HSC Report acknowledged that the eligibility criteria differ between Whaikaha and Te Whatu Ora-funded services, resulting in inequitable access.
The Report also states that a person does not require a classified disability to access health services, however in practice ANZMES has found that many with ME/CFS are denied help, despite the obvious need. ANZMES understand that support needs to be prioritised but at present, due to a misconception around the severity of the illness and the lack of functionality that results, many are seen as low on the priority scale.
ANZMES plans to continue to discuss this with the government and Whaikaha and would like them to consider working together to improve current assessment pathways and streamline the process to reduce access inequity across the country.
People with this debilitating condition face a barrier to support under the current classification of “chronic illness” and as a result experience poor quality of life and health inequity. With increasing numbers of people with long COVID (LC) being diagnosed with ME/CFS the existing support through nonprofit organisations is set to become unmanageable, with case numbers still rising.
People with ME want to see the actual implementation of these recommendations. Practical help is urgently needed for this growing under-supported, disabled community that could lead to a better prognosis and better quality of life.
To view the full report:
HSC-2022-Final-report-Petition-of-ANZMES——————————————————————————–
What is ME/CFS?
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is often triggered by a viral illness and involves overwhelming fatigue and other symptoms that range in severity as it affects many body systems, such as the immune, neuroendocrine and autonomic nervous system.
The key characteristic of ME/CFS is post exertional malaise (PEM) which presents 12-48 hours after exertion, and can result in days to weeks of exacerbated symptoms. For the very severe, this exertion can be simply trying to speak, or eat.
Who are ANZMES?
The Associated New Zealand ME Society (ANZMES) has been providing information, awareness for ME, funding research, and advocating for people with ME for the past 43 years (since 1980). As the National Advisory on ME in Aotearoa/New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME voice globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership. ANZMES is a RNZCGP registered provider for continuing education. Health professionals can earn CME/CPD credits with ANZMES latest education programme – Know M.E. – a video podcast and news series featuring up-to-date, evidence based research and information on ME/CFS and Post COVID Conditions.
————————————————————————————-
For more information contact
info@anzmes.org.nz

BenefitMe is a new website aimed at helping people find what benefits they can receive.
There are lots of Work and Income benefits for people who need help in Aotearoa New Zealand, but it can be hard to know which ones you can get. BenefitMe helps you find out what you’re eligible for and what happens if things in your life change.
BenefitMe is a community effort to put some power back into the hands of the public, so anyone can find the support and services they’re legally eligible for and be more able to engage from a position of confidence with government departments.
Payments currently supported:
BenefitMe is an initiative by the Digital Aotearoa Collective (DAC), a civil society group committed to addressing injustice and improving wellbeing in Aotearoa New Zealand. Click the link to find more about BenefitMe

PRESS RELEASE – for immediate release
If you’ve never heard of post-exertional malaise (PEM) you’re not alone. But for people living with ME/CFS or long Covid understanding PEM is crucial to managing their illness. World ME Day on May 12 is an opportunity to increase your understanding of this little-known phenomenon.
Post-exertional malaise (PEM) is something that everyone with ME/CFS (Myalgic Encephalomyelitis /Chronic Fatigue Syndrome) experiences. So what is it? Put simply, PEM is a debilitating and abnormal response to normal activity.
People with ME/CFS and long COVID have what is called an energy envelope. This is the amount of energy they have on any given day to function. Research and experience shows that if a person expends an equivalent amount of energy to the amount they have available they will reduce the symptom flares they experience.
When people with ME/CFS and long COVID push to do more than their energy envelope can cope with, the severity of their symptoms increase. This period of reduced functionality and exacerbation of symptoms typically starts within 12 to 48 hours after the activity or exposure and may last for days, weeks, or may also be permanent.
When PEM hits, people report existing symptoms increase, and that new ones appear including brain fog (executive functioning), flu-like symptoms (sore throat, muscle pain, increased fatigue); muscle weakness; increased sensitivity to noise, light or touch; pain; sleep problems.
How much and what type of exertion triggers PEM is different for each person. Triggers can include:
Leading ME/CFS researcher Dr Lynette Hodges, Exercise Physiologist, Massey University, says “Individuals with ME/CFS are not lazy or deconditioned. Our research has shown physiological changes for those with ME/CFS. Both planned exercise and even simple activities of daily living can cause PEM.”
PEM is best managed by creating an individualised routine of rest and carefully paced activities within the individual’s current energy envelope. GP Cathy Stephenson states “If there’s one thing to impress upon health providers when it comes to the management of ME/CFS, it’s Pacing. Above all else. Pacing.”
Kate was diagnosed with ME 5 years ago after 20 plus years of health challenges triggered from a viral illness. Before this she was hardly ever sick, a school prefect, and played high level sport representing New Zealand for Water Polo. In 2018 her system crashed after pushing through symptoms for too long when numerous doctors weren’t able to help. She suffered with crushing fatigue that did not improve after a full night’s sleep and had to give up work, sports and her social life. She was mostly confined to her home, except for dropping off and picking up her boy from daycare/school and other activities.
She also experienced constant body pain, fluctuating headaches, neurological problems resulting in impaired memory and an inability to concentrate and Postural Orthostatic Tachycardia Syndrome (POTS), a dysfunction in the autonomic nervous system. Any physical, mental, or emotional effort would cause worsening of her symptoms and she had to learn to work within a very small energy envelope.
Five years on, Kate has made what is known as significant progress in the ME community, with a reduction in symptoms enough that she can work a small number of hours each week. She can attend more activities with her son, however her dreams of dancing and playing masters level competitive sports are not fulfilled and she is accepting that she may never reach these and other dreams she has.

Visit the World ME Day information from ANZMES on https://anzmes.org.nz/worldmeday2023/
Follow the Learn From ME page on Facebook on May 12th to follow the World ME Day campaign. This page is a collaborative initiative between the regional and national ME/CFS organisations:
ANZMES (Associated NZ ME Societies)
Complex Chronic Illness Support
ME Support
MECFS Canterbury
MEISS Otago
ME Awareness NZ
Rest Assured Respite Trust
Find out more about ME/CFS or to take action to support World ME Day by visiting: www.worldmeday.org

ANZMES is set to speak to parliament on May 3rd to present an oral submission to the Health Committee – an opportunity to strengthen the argument for the reclassification of ME/CFS to a disability.
Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) petition to reclassify ME/CFS as a disability was read in Parliament, on the 13th of September 2022, and has been under consideration with the Health Committee since then.
ANZMES president, Fiona Charlton, will speak to parliament on behalf of the members that she represents, along with Emeritus Professor Warren Tate and RCNZGPs Fellow Dr. Sarah Dalziel, who will answer the committee’s questions.
ME/CFS is a debilitating long term condition that affects multiple body systems and is characterised by Post Exertional Malaise, where symptoms worsen after periods of even ordinary activities. The current classification of ME/CFS as an illness rather than a disability makes it difficult for individuals who suffer from the condition to access the necessary support that they need to lead quality lives.
“We must make this chronic condition a disability now and give people fair access to the help that they need,” says Charlton.
A growing number of people with long COVID are now being diagnosed with ME/CFS, putting strain on already exhausted resources.
There is no dedicated funding for the condition and the current classification and system is difficult to navigate. There are complicated assessment processes and policies. There is disparity between regions causing access inequality.
In order to be diagnosed with ME/CFS a person must be significantly impaired in terms of functioning in daily life, such as work or school.
ANZMES has presented the government with detailed reports, research and recommendations and now hope that they will listen and take the urgent action that is needed.
Reclassification will lead to real improvements for those in need; providing access to disability support services – much needed home help, housing support, financial support, and counselling access.

What is ME/CFS?
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is often triggered by a viral illness and involves overwhelming fatigue and other symptoms that range in severity as it affects many body systems, such as the immune, neuroendocrine and autonomic nervous system.
The key characteristic of ME/CFS is post exertional malaise (PEM) which presents 12-48 hours after exertion, and can result in days to weeks of exacerbated symptoms. For the very severe, this exertion can be simply trying to speak, or eat.
Who are ANZMES?
The Associated New Zealand Society for ME/CFS (ANZMES) have been providing information, awareness for ME/CFS, funding research, and advocating for people with ME/CFS for the past 43 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership. ANZMES is a RNZCGP registered provider for continuing education. Health professionals can earn CME/CPD credits with ANZMES latest education programme – Know M.E. – a video podcast and news series featuring up-to-date, evidence based research and information on ME/CFS and Post COVID Conditions.
For more information contact
info@anzmes.org.nz

Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) is calling for ME/CFS to be reclassified as a disability.
We urge you to to pledge your support for this change.
People with this debilitating condition face a barrier to support under the current classification of “chronic illness” and as a result experience poor quality of life and health inequity. With increasing numbers of people with Long COVID (LC) being diagnosed with ME/CFS the existing support through nonprofit organisations is set to become unmanageable, with case numbers still rising.
With the new Whaikaha – Ministry of Disabled People still in development ANZMES sees that this is a timely opportunity to move forward with this long overdue change.
ANZMES President, Fiona Charlton says, “it is vital for ME/CFS and LC that this access is improved. “Many people have symptoms that are so severe that they struggle with daily tasks like showering, making a meal and are bedbound or require a wheelchair. “This growing community of chronically ill people deserve better treatment and urgently need more access to financial support and health services with acknowledgment that their illness is disabling.”


Despite the symptoms of ME/CFS meeting many of the definitions for disability, the illness is not categorised as a disability in New Zealand for the purpose of health-related funding and support.
The Human Rights Act 1993 states that disability can be defined as:
Physical disability or impairment: physical illness: psychiatric illness: intellectual or psychological
disability or impairment: any other loss or abnormality of psychological, physiological: or anatomical
structure or function: reliance on a guide dog, wheelchair, or other remedial means: the presence in the
body of organisms capable of causing illness.
Reclassification will lead to real improvements in quality of life for those in need. Some people with ME/CFS become ill and never return to their pre-illness capabilities – this makes the condition life-long. ME/CFS patients require home help, housing support, financial support, and counselling access. Many people, following COVID-19 infection, are being diagnosed with ME/CFS and also require ongoing support services.


Reclassification of ME/CFS to disability would result in:
What is ME/CFS?
A chronic illness involving overwhelming ongoing fatigue, ME/CFS is often triggered by a viral illness. The condition causes a variety of symptoms that range in severity as it affects many body systems, such as the immune, neuroendocrine and autonomic nervous system.
Who are ANZMES?
ANZMES has been providing information, building awareness, funding research, and advocating for people with ME/CFS for the past 42 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership.
ANZMES urges you to join us in supporting this petition by signing and sharing with your networks: https://www.parliament.nz/en/pb/petitions/document/PET_125649/petition-of-associated-myalgic-encephalomyelitis-society

– no endorsement for Lightning Process for ME
The Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) supports the new position paper on the Lightning Process by the World ME Alliance and does not endorse the Lightning Process for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).
The Lightning Process is a programme loosely based on concepts of neuro linguistic programming (NLP) and cognitive behaviour therapy (CBT) that is set up commercially and currently marketed as a cure for ME/CFS. This claim is not backed by scientific evidence and ANZMES shares the view of the World ME Alliance that the promotion of this programme is likely to do harm.
The National Institute for Health and Care Excellence (NICE), in the UK, revised their guidelines for the diagnosis, treatment, and management of ME/CFS stating that the lightning process should not be used as a treatment and they no longer recommend CBT. These changes reflect a shift from an outdated perspective that ME/CFS was a psychological condition and follows evidence from over 200 studies showing poor efficacy for this treatment approach.
ANZMES President, Fiona Charlton says, “there is a growing body of evidence that shows that ME is driven by physiological changes not psychological ones and telling people that they can talk themselves out of this condition, within three days, could be very harmful.
“We know that if people with ME ignore their symptoms and push themselves this can make things worse, sometimes to the point of needing hospital care.”
ANZMES agrees with the World ME Alliance who highlight in their statement that people with ME/CFS are vulnerable to exploitation due to a lack of effective treatment where programmes like the Lightning Process are just filling this void.
People living with Long COVID are also being drawn into this treatment as this is now an extension of their claims to cure ME/CFS.
Other concerns with the Lightning Process include a bias in efficacy studies, including conflicts of interest, a reported secrecy where participants are told not to speak about the programme or their symptoms and a level of shame and guilt for those who do not recover within the three days of treatment.
Charlton says, “we want to ensure that if we are endorsing a treatment for ME that robust evidence supports efficacy and this is just not the case with LP.
“What we do know is that a treatment approach that is focussed around symptom management is shown to help with the relapsing nature of ME.”
ANZMES acknowledges that neurological symptoms, such as depression and anxiety can be a part of ME/CFS and may benefit from supportive therapies but people have the right to unbiased, impartial information when being offered these treatments.
***********************
The Lightning Process was developed and trademarked by British osteopath and hypnotherapist Phil Parker.
ANZMES has been providing information, building awareness, funding research, and advocating for people with ME/CFS for the past 42 years (since 1980). As the national advisory body for ME/CFS in New Zealand, ANZMES disseminates evidence-based information nationally, and represents the ME/CFS voice, globally as a founding member of the World ME Alliance. ANZMES acts as the voice of all people living with this disabling disease through advocacy and leadership.
Position Statement World ME Alliance
NICE Guidelines
Contact ANZMES for more information

The World ME Alliance, a collaborative of organisations from across the globe, is launching World ME Day on 12th May this year. This new initiative aims to bring together organisations and unify efforts to raise awareness and campaign together on Myalgic Encephalomyelitis (ME). Through collective action, we will step closer to our goal of a world without ME.
World ME Day will build on the incredible efforts of advocates around events, such as ME Awareness Week and Chronic Immunological and Neurological Diseases (CIND) Awareness Day. By focusing on a single day and collaborating across many organisations, we aim to maximise our collective power.
The theme for the first year of World ME Day is #LearnFromME.
Read More: here

What should the world #LearnFromME?
ME is a global health crisis – up to 30 million people are living with this disease worldwide, and when we take into account the effect on families, carers and friends too, the impact of this disease cannot be overstated.
But there is much to be learnt from this disease – from the willpower and determination of those living with it, to the incredible advocates working towards change, to an understanding that the most meaningful change will comes from high-quality research.
We want to use World ME Day to reach out to health professionals on a personal basis, build understanding of ME and take another step towards a world that understands ME.
Read more: here
At the request of the ME/CFS community, ANZMES has issued a survey relating to reactions experienced by the community to the COVID-19 Pfizer BioNTech vaccine. ANZMES also sought to ascertain prevalence of Long COVID and COVID-19 infection in the community. The opportunity was also utilised for respondents to express interest in participating in a potential fractionated dosing trial.
This report contains preliminary findings for responses received from 21st October 2021 to 10th November 2021. This survey is still open to capture experiences after these dates, as vaccination decisions are ongoing.
Please note that this survey is classed as a self-report questionnaire which seeks to ascertain the subjective experience of people with ME/CFS and co-morbid conditions. The information collected is therefore anecdotal data. No clinical research has been conducted.
The majority of respondents have a clinical diagnosis of ME, with 25 self-diagnosed. Most are unsure as to which diagnostic criteria for ME was used.
Some questions have less respondents, therefore numbers are indicated in the relevant sections.
The majority of respondents have had two doses of the Pfizer vaccination.
Of the 296 with two doses, the duration between doses was 6 weeks or more for 166 individuals and 3 weeks for 130.
These findings suggest that the more disabling the ME/CFS symptoms, the more prone to a relapse after vaccination but that relapse can occur at any functional capacity state for pwME. This was analysed when there were 241 responses.
| Temporarily worsened | Improved | No change | Worsened into relapse | Worsened beyond illness | Not vaccinated | No answer | |
| Part-time work home | 22 | 8 | 7 | 9 | 1 | 14 | 2 |
| Part-time outside house | 22 | 3 | 17 | 14 | 0 | 12 | 2 |
| Full-time work mild-mod with activity ME FM Long COVID/COVID | 3 2 0 | 0 0 2 | 4 1 3 | 3 1 0 | 0 0 0 | 2 0 1 | 2 0 5 |
| Unable to work, confined to house | 23 | 6 3 temp | 15 | 18 | 7 | 8 | 7 |
| Bedbound mostly | 2 | 0 | 0 | 3 | 0 | 1 | 1 |
| Bedbound unable to care for self | 0 | 0 | 0 | 1 | 0 | 1 | 1 |
| Overall ME | 72 | 20 | 43 | 48 | 8 | 30 | 20 |
There were 39 individuals who did not experience any symptoms. For those who did experience reactions to the first dose of the vaccine, these were consistent with the expected normal immune response, e.g.:
5 people experienced heart palpitations and/or anxiety 3 people experienced skin sensitivity and/or allergy flares, with 2 people experiencing brain fog/cognitive issues.
As has been reported by the general public, the findings from this survey suggest that pwME also experienced more adverse reactions to the second dose of the Pfizer vaccine. However there were 54 individuals who did not experience any symptoms.
2 experienced skin sensitivity, 2 experienced fibromyalgia flare-ups, 2 experienced palpitations and/or anxiety symptoms, 2 experienced brain fog/cognitive issues.
289 respondents did not have any new symptoms that they could attribute to the vaccine.
52 stated that they had new symptoms that they could attribute to the vaccine. These symptoms tended to be over-activation of the immune response, e.g. sore throat, swollen neck glands, allergy reactions. Of these 52 – 4 individuals have gastrointestinal issues, 2 experienced more fatigue whilst 1 indicated improved energy.
From 383 responses 314 (82%) were not offered clinical care during vaccination, 15 (3.9%) were offered clinical care, 19 (5%) were unsure. 25 people asked for specific clinical care during the vaccination process. Of those offered clinical care the options were 30 minute observation rather than the normal 15, separate areas with direct nurse observation. Others were advised by their GPs to rest and take antihistamines pre- and post-vaccination.
From 353 respondents 50 require ongoing caregiving for their ME/CFS and/or FM and 70 required care after vaccination. 244 people do not require caregiving before and 230 after.
If fractionated / lower dosing had been an option, of 115 responses 48 stated they would have considered it, 23 said they would not consider it and 44 were unsure.
Of 88 responses for those reluctant to have the vaccine, 57 would consider lower dosing options, 10 would not, and 21 were unsure.
Of 124 responses to indicate interest in participation in a potential trial into fractionated dosing, 61 responded that they are interested, 31 may be interested, and 32 are not.
Of 115 responses 45 did not take any pre- or post-vaccination, 70 did.
Of 1Anxiety/worry/fear about potential adverse reactions, previous adverse reactions to other vaccines, concern about the safety of the vaccine, high ME/CFS symptomatology, chemical sensitivities/MCS/MCAS, not currently well enough to risk adverse reactions.
19 respondents have been diagnosed with SARS-CoV-2 (COVID-19) infection.
169 respondents have had COVID-19 tests.
5 people have been diagnosed by a medical professional with Long COVID.
32 people suspected they have Long COVID after a viral infection due to ongoing or lingering classic COVID-19 symptoms and having been connected to a location of interest, an overseas hot zone of infection, or have remained unwell after experiencing a viral infection that has not been confirmed as COVID but has the same symptoms.
Symptoms by response from 57 individuals:
From 57 responses
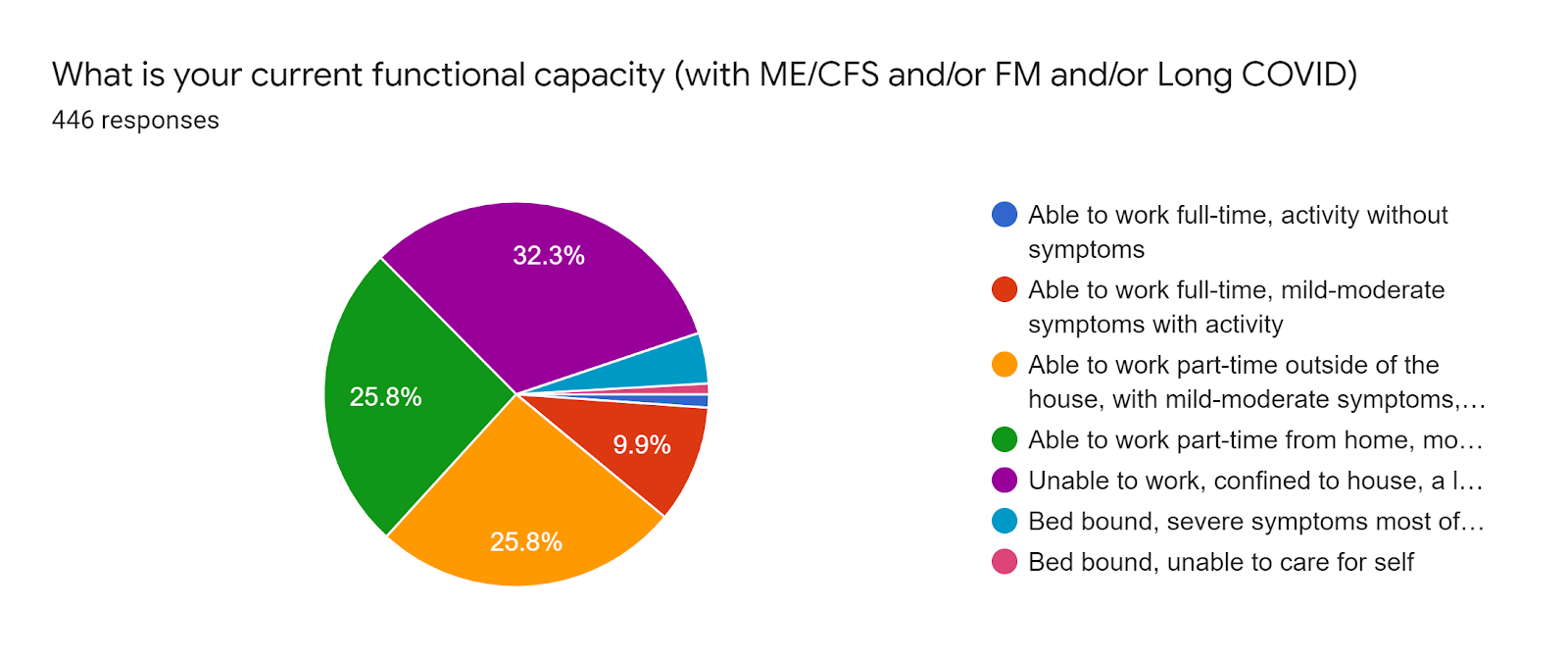
From 447 responses, respondents identify as:
Age range from 453 responses:
From 447 responses, respondents live in the following regions: